Greenhalgh Trisha, A'Court Christine, Shaw Sara
Nuffield Department of Primary Care Health Sciences, University of Oxford, Radcliffe Primary Care Building, Woodstock Rd, Oxford, OX2 6GG, UK.
BMC Cardiovasc Disord. 2017 Jun 14;17(1):156. doi: 10.1186/s12872-017-0594-2.
Enthusiasts for telehealth extol its potential for supporting heart failure management. But randomised trials have been slow to recruit and produced conflicting findings; real-world roll-out has been slow. We sought to inform policy by making sense of a complex literature on heart failure and its remote management.
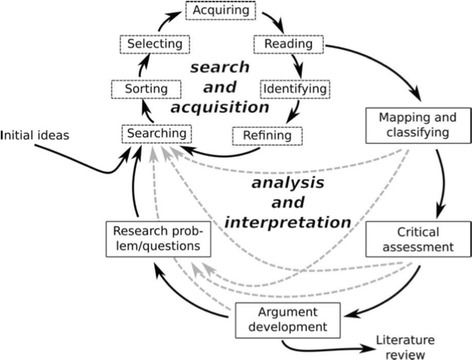
Through database searching and citation tracking, we identified 7 systematic reviews of systematic reviews, 32 systematic reviews (including 17 meta-analyses and 8 qualitative reviews); six mega-trials and over 60 additional relevant empirical studies and commentaries. We synthesised these using Boell's hermeneutic methodology for systematic review, which emphasises the quest for understanding.
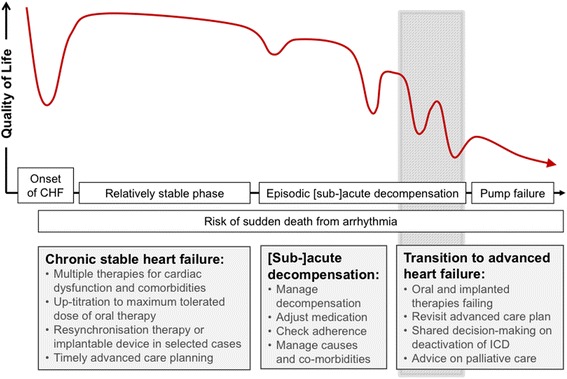
Heart failure is a complex and serious condition with frequent co-morbidity and diverse manifestations including severe tiredness. Patients are often frightened, bewildered, socially isolated and variably able to self-manage. Remote monitoring technologies are many and varied; they create new forms of knowledge and new possibilities for care but require fundamental changes to clinical roles and service models and place substantial burdens on patients, carers and staff. The policy innovation of remote biomarker monitoring enabling timely adjustment of medication, mediated by "activated" patients, is based on a modernist vision of efficient, rational, technology-mediated and guideline-driven ("cold") care. It contrasts with relationship-based ("warm") care valued by some clinicians and by patients who are older, sicker and less technically savvy. Limited uptake of telehealth can be analysed in terms of key tensions: between tidy, "textbook" heart failure and the reality of multiple comorbidities; between basic and intensive telehealth; between activated, well-supported patients and vulnerable, unsupported ones; between "cold" and "warm" telehealth; and between fixed and agile care programmes.
The limited adoption of telehealth for heart failure has complex clinical, professional and institutional causes, which are unlikely to be elucidated by adding more randomised trials of technology-on versus technology-off to an already-crowded literature. An alternative approach is proposed, based on naturalistic study designs, application of social and organisational theory, and co-design of new service models based on socio-technical principles. Conventional systematic reviews (whose goal is synthesising data) can be usefully supplemented by hermeneutic reviews (whose goal is deepening understanding).
远程医疗的支持者称赞其在支持心力衰竭管理方面的潜力。但随机试验的招募工作进展缓慢,结果也相互矛盾;实际推广也很缓慢。我们试图通过梳理关于心力衰竭及其远程管理的复杂文献来为政策提供参考。
通过数据库检索和引文跟踪,我们识别出7篇系统评价的系统评价、32篇系统评价(包括17篇荟萃分析和8篇定性评价);6项大型试验以及60多项其他相关实证研究和评论。我们使用博埃尔的诠释学系统评价方法对这些进行综合分析,该方法强调对理解的追求。
心力衰竭是一种复杂且严重的疾病,常伴有多种合并症,表现多样,包括严重疲劳。患者通常感到恐惧、困惑, 社交孤立,自我管理能力也各不相同。远程监测技术种类繁多;它们创造了新的知识形式和护理新可能,但需要对临床角色和服务模式进行根本性变革,给患者、护理人员和工作人员带来巨大负担。由 “积极主动” 的患者介导的远程生物标志物监测这一政策创新,能够及时调整药物治疗,其基于一种现代主义的高效、理性、技术介导和指南驱动(“冷漠”)护理愿景。这与一些临床医生以及年龄较大、病情较重且技术不太熟练的患者所重视的基于关系的(“温暖”)护理形成对比。远程医疗采用率有限可从以下关键矛盾方面进行分析:整齐划一的 “教科书式” 心力衰竭与多种合并症现实之间的矛盾;基础远程医疗与强化远程医疗之间的矛盾;积极主动、得到充分支持的患者与脆弱、缺乏支持的患者之间的矛盾;“冷漠” 与 “温暖” 远程医疗之间的矛盾;以及固定护理方案与灵活护理方案之间的矛盾。
心力衰竭远程医疗采用率有限存在复杂的临床、专业和机构原因,在本就繁多的文献中增加更多技术开启与技术关闭的随机试验不太可能阐明这些原因。我们提出了一种替代方法,基于自然主义研究设计、社会和组织理论的应用以及基于社会技术原则的新服务模式的共同设计。传统的系统评价(其目标是综合数据)可以通过诠释学评价(其目标是深化理解)得到有效补充。