Sonnappa Samatha, Martin Richard, Israel Elliot, Postma Dirkje, van Aalderen Wim, Burden Annie, Usmani Omar S, Price David B
Observational and Pragmatic Research Institute Pte Ltd, Singapore, Singapore.
Department of Respiratory Paediatrics, Rainbow Children's Hospital, Bengaluru, India.
PLoS One. 2017 Jun 15;12(6):e0178112. doi: 10.1371/journal.pone.0178112. eCollection 2017.
Regular use of inhaled corticosteroids (ICS) in patients with obstructive lung diseases has been associated with a higher risk of pneumonia, particularly in COPD. The risk of pneumonia has not been previously evaluated in relation to ICS particle size and dose used.
Historical cohort, UK database study of 23,013 patients with obstructive lung disease aged 12-80 years prescribed extra-fine or fine-particle ICS. The endpoints assessed during the outcome year were diagnosis of pneumonia, acute exacerbations and acute respiratory events in relation to ICS dose. To determine the association between ICS particle size, dose and risk of pneumonia in unmatched and matched treatment groups, logistic and conditional logistic regression models were used.
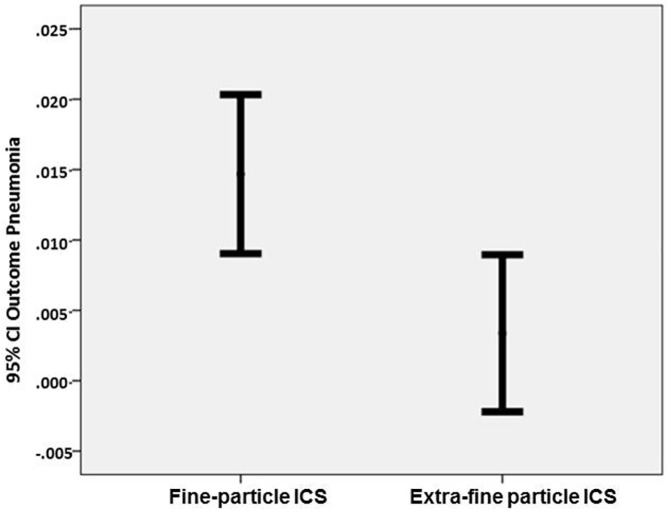
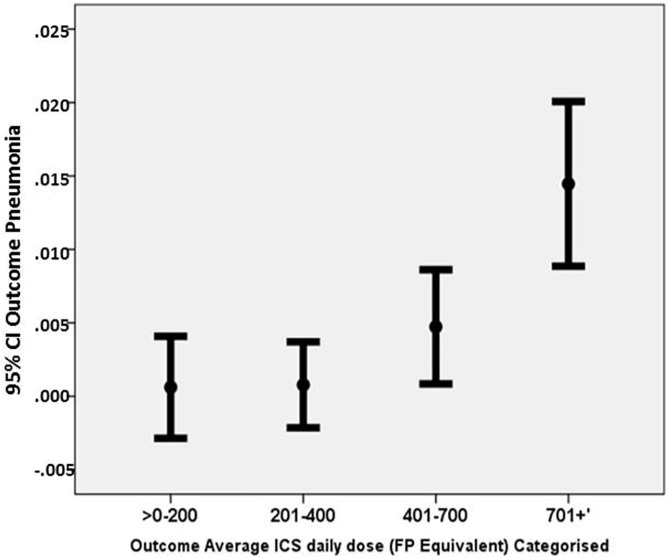
14788 patients were stepped-up to fine-particle ICS and 8225 to extra-fine ICS. On unmatched analysis, patients stepping-up to extra-fine ICS were significantly less likely to be coded for pneumonia (adjusted odds ratio [aOR] 0.60; 95% CI 0.37, 0.97]); experience acute exacerbations (adjusted risk ratio [aRR] 0.91; 95%CI 0.85, 0.97); and acute respiratory events (aRR 0.90; 95%CI 0.86, 0.94) compared with patients stepping-up to fine-particle ICS. Patients prescribed daily ICS doses in excess of 700 mcg (fluticasone propionate equivalent) had a significantly higher risk of pneumonia (OR [95%CI] 2.38 [1.17, 4.83]) compared with patients prescribed lower doses, irrespective of particle size.
These findings suggest that patients with obstructive lung disease on extra-fine particle ICS have a lower risk of pneumonia than those on fine-particle ICS, with those receiving higher ICS doses being at a greater risk.
在患有阻塞性肺病的患者中,长期使用吸入性糖皮质激素(ICS)与肺炎风险升高相关,尤其是在慢性阻塞性肺疾病(COPD)患者中。此前尚未针对ICS的颗粒大小和使用剂量对肺炎风险进行评估。
这是一项基于英国数据库的历史性队列研究,纳入了23013名年龄在12至80岁之间、正在使用超细或细颗粒ICS的阻塞性肺病患者。在随访年度评估的终点指标包括与ICS剂量相关的肺炎诊断、急性加重和急性呼吸事件。为了确定在未匹配和匹配治疗组中ICS颗粒大小、剂量与肺炎风险之间的关联,使用了逻辑回归和条件逻辑回归模型。
14788名患者升级使用细颗粒ICS,8225名患者升级使用超细颗粒ICS。在未匹配分析中,升级使用超细颗粒ICS的患者被编码为肺炎的可能性显著更低(调整后的优势比[aOR]为0.60;95%置信区间[CI]为0.37,0.97);发生急性加重的可能性(调整后的风险比[aRR]为0.91;95%CI为0.85,0.97);以及急性呼吸事件的可能性(aRR为0.90;95%CI为0.86,0.94),与升级使用细颗粒ICS的患者相比。无论颗粒大小如何,每日ICS剂量超过700微克(丙酸氟替卡松等效剂量)的患者患肺炎的风险显著更高(OR[95%CI]为2.38[1.17,4.83]),与使用较低剂量的患者相比。
这些发现表明,使用超细颗粒ICS的阻塞性肺病患者患肺炎的风险低于使用细颗粒ICS的患者,而接受较高ICS剂量的患者风险更大。