Department of Medicine, David Geffen School of Medicine, University of California Los Angeles, 10833 Le Conte Avenue, Los Angeles, CA, 90095-1690, USA.
Pneumology Department, Hospital Universitari Vall d'Hebron, CIBER de Enfermedades Respiratorias (CIBERES), Barcelona, Spain.
Respir Res. 2018 Oct 5;19(1):196. doi: 10.1186/s12931-018-0874-0.
Use of inhaled corticosteroids (ICS) increases the risk of pneumonia in chronic obstructive pulmonary disease (COPD), but the magnitude of risk with different ICS remains unclear.
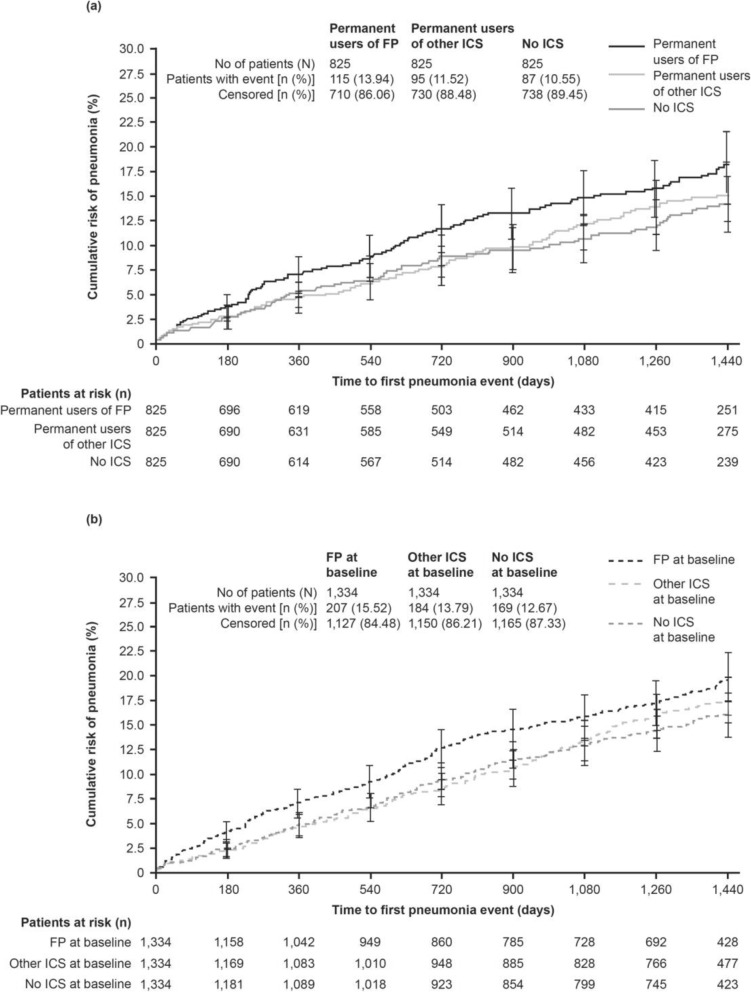
A post hoc analysis of the 4-year UPLIFT® trial to assess whether pneumonia risk differed by type of ICS (fluticasone propionate [FP], other ICS, or no ICS) in permanent users (defined by use until end of study) or in users at baseline (sensitivity analysis).
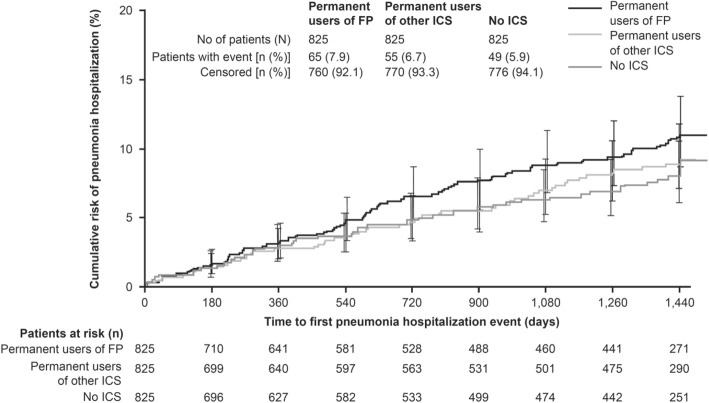
For the permanent-users analysis, 825 patients receiving FP throughout the trial, 825 patients receiving other ICS and 825 patients not receiving ICS were matched on relevant baseline features 1:1:1. A significantly greater risk of pneumonia was observed for FP versus no ICS: the hazard ratio (HR) for risk of pneumonia was 1.33 (95% confidence interval [CI] 1.00, 1.75; p = 0.046) and the rate ratio (RR) was 1.58 (95% CI 1.05, 2.37; p = 0.028). A greater risk was also found for FP versus other ICS: HR 1.28 (95% CI 0.97, 1.68; p = 0.078) and RR 1.48 (95% CI 1.00, 2.19; p = 0.049). A higher proportion of patients on FP were hospitalized with pneumonia (7.9%) versus other ICS (6.7%) or no ICS (5.9%). Whilst other ICS use was associated with the highest number of fatal pneumonia events, the total number of fatal pneumonia incidents was low. A similar pattern was observed in the sensitivity analyses, which included 4002 patients on different treatments at baseline (FP, other ICS, and no ICS) and considered potential switches during the study.
The results support existing evidence of an increased pneumonia risk with FP use compared with other ICS and no ICS use in patients with COPD. Healthcare professionals should evaluate the risk-benefit ratio of using ICS when making treatment decisions with their patients.
Post hoc analysis of UPLIFT®. ClinicalTrials.gov number: NCT00144339 . Retrospectively registered September 2, 2005.
在慢性阻塞性肺疾病(COPD)患者中,使用吸入性皮质类固醇(ICS)会增加肺炎的风险,但不同 ICS 的风险程度尚不清楚。
对为期 4 年的 UPLIFT®试验进行了事后分析,以评估在永久性使用者(定义为研究结束前一直使用)或基线使用者(敏感性分析)中,ICS 类型(丙酸氟替卡松[FP]、其他 ICS 或无 ICS)是否会导致肺炎风险不同。
对于永久性使用者分析,在整个试验中接受 FP 的 825 名患者、接受其他 ICS 的 825 名患者和未接受 ICS 的 825 名患者按相关基线特征进行了 1:1:1 匹配。与无 ICS 相比,FP 治疗的肺炎风险显著增加:肺炎风险的危险比(HR)为 1.33(95%置信区间[CI]为 1.00,1.75;p=0.046),比率比(RR)为 1.58(95%CI 为 1.05,2.37;p=0.028)。FP 与其他 ICS 相比也有更高的风险:HR 1.28(95%CI 为 0.97,1.68;p=0.078),RR 1.48(95%CI 为 1.00,2.19;p=0.049)。FP 组发生肺炎住院的患者比例(7.9%)高于其他 ICS(6.7%)或无 ICS(5.9%)。尽管其他 ICS 治疗与最高数量的致命性肺炎事件相关,但致命性肺炎事件的总数仍然较低。在敏感性分析中也观察到了类似的模式,该分析包括了基线时接受不同治疗(FP、其他 ICS 和无 ICS)的 4002 名患者,并考虑了研究期间的潜在转换。
这些结果支持现有证据,即与其他 ICS 和无 ICS 相比,COPD 患者使用 FP 会增加肺炎风险。当为患者做出治疗决策时,医疗保健专业人员应评估使用 ICS 的风险效益比。
UPLIFT®的事后分析。ClinicalTrials.gov 编号:NCT00144339。2005 年 9 月 2 日进行了回顾性注册。