Saunders Peter, Tsipouri Vicky, Keir Gregory J, Ashby Deborah, Flather Marcus D, Parfrey Helen, Babalis Daphne, Renzoni Elisabetta A, Denton Christopher P, Wells Athol U, Maher Toby M
NIHR Biomedical Research Unit, Royal Brompton Hospital, Sydney Street, London, SW3 6NP, UK.
Princess Alexandra Hospital, Brisbane, QLD, Australia.
Trials. 2017 Jun 15;18(1):275. doi: 10.1186/s13063-017-2016-2.
Interstitial lung disease (ILD) frequently complicates systemic autoimmune disorders resulting in considerable morbidity and mortality. The connective tissue diseases (CTDs) most frequently resulting in ILD include: systemic sclerosis, idiopathic inflammatory myositis (including dermatomyositis, polymyositis and anti-synthetase syndrome) and mixed connective tissue disease. Despite the development, over the last two decades, of a range of biological therapies which have resulted in significant improvements in the treatment of the systemic manifestations of CTD, the management of CTD-associated ILD has changed little. At present there are no approved therapies for CTD-ILD. Following trials in scleroderma-ILD, cyclophosphamide is the accepted standard of care for individuals with severe or progressive CTD-related ILD. Observational studies have suggested that the anti-CD20 monoclonal antibody, rituximab, is an effective rescue therapy in the treatment of refractory CTD-ILD. However, before now, there have been no randomised controlled trials assessing the efficacy of rituximab in this treatment population.
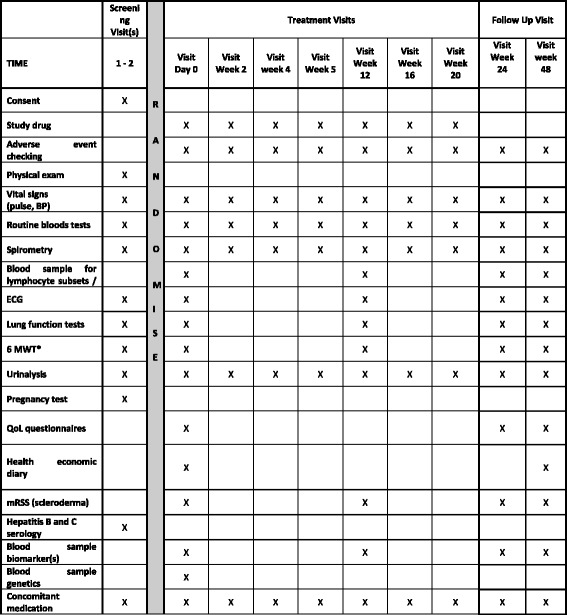
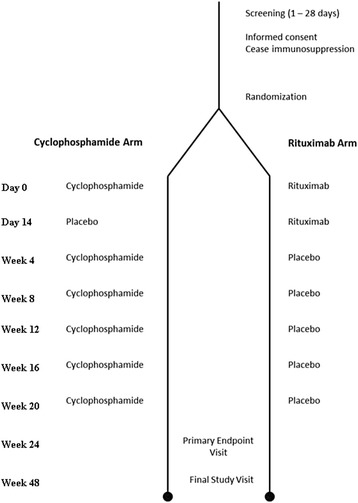
METHODS/DESIGN: RECITAL is a UK, multicentre, prospective, randomised, double-blind, double-dummy, controlled trial funded by the Efficacy and Mechanism Evaluation Programme of the Medical Research Council and National Institute for Health Research. The trial will compare rituximab 1 g given intravenously, twice at an interval of 2 weeks, with intravenously administered cyclophosphamide given monthly at a dose of 600 mg/m body surface area in individuals with ILD due to systemic sclerosis, idiopathic inflammatory myositis (including anti-synthetase syndrome) or mixed connective tissue disease. A total of 116 individuals will be randomised 1:1 to each of the two treatment arms, with stratification based on underlying CTD, and will be followed for a total of 48 weeks from first dose. The primary endpoint for the study will be change in forced vital capacity (FVC) at 24 weeks. Key secondary endpoints include: safety, change in FVC at 48 weeks as well as survival, change in oxygen requirements, total 48-week corticosteroid exposure and utilisation of health care resources.
This is the first randomised control trial to study the efficacy of rituximab as first-line treatment in CTD-associated ILD. The results generated should provide important information on the treatment of a life-threatening complication affecting a rare group of CTDs.
ClinicalTrials.gov, NCT01862926. Registered on 22 May 2013.
间质性肺病(ILD)常并发于系统性自身免疫性疾病,导致较高的发病率和死亡率。最常引发ILD的结缔组织病(CTD)包括:系统性硬化症、特发性炎性肌病(包括皮肌炎、多发性肌炎和抗合成酶综合征)以及混合性结缔组织病。尽管在过去二十年中开发了一系列生物疗法,使CTD的全身表现治疗有了显著改善,但CTD相关ILD的管理变化不大。目前尚无获批用于CTD-ILD的疗法。在硬皮病-ILD试验之后,环磷酰胺是重度或进行性CTD相关ILD患者公认的标准治疗方法。观察性研究表明,抗CD20单克隆抗体利妥昔单抗是治疗难治性CTD-ILD的有效挽救疗法。然而,在此之前,尚无随机对照试验评估利妥昔单抗在该治疗人群中的疗效。
方法/设计:RECITAL是一项由医学研究理事会疗效与机制评估计划和国家卫生研究院资助的英国多中心、前瞻性、随机、双盲、双模拟对照试验。该试验将比较静脉注射1g利妥昔单抗,每2周一次,共两次,与静脉注射环磷酰胺,每月一次,剂量为600mg/m²体表面积,用于因系统性硬化症、特发性炎性肌病(包括抗合成酶综合征)或混合性结缔组织病导致ILD的患者。总共116名患者将按1:1随机分配到两个治疗组,根据潜在的CTD进行分层,从首次给药起共随访48周。该研究的主要终点将是24周时用力肺活量(FVC)的变化。关键次要终点包括:安全性、48周时FVC的变化以及生存率、氧气需求变化、48周内皮质类固醇总暴露量和医疗资源利用情况。
这是第一项研究利妥昔单抗作为CTD相关ILD一线治疗疗效的随机对照试验。产生的结果应为治疗影响罕见CTD群体的危及生命并发症提供重要信息。
ClinicalTrials.gov,NCT01862926。于2013年5月22日注册。