Bally Julien F, Vargas Maria-Isabel, Horvath Judit, Fleury Vanessa, Burkhard Pierre, Momjian Shahan, Pollak Pierre, Boex Colette
Department of Neurology, University Hospitals of Geneva (HUG), Geneva, Switzerland.
Department of Neurology, Movement Disorders Research Center, Toronto Western Hospital, University of Toronto, Toronto, ON, Canada.
Front Neurol. 2017 May 31;8:239. doi: 10.3389/fneur.2017.00239. eCollection 2017.
Successful deep brain stimulation (DBS) in Parkinson's disease (PD) requires optimal electrode placement. One technique of intraoperative electrode testing is determination of stimulation thresholds inducing corticospinal/corticobulbar tracts (CSBT) motor contractions.
This study aims to analyze correlations between DBS electrode distance to CSBT and contraction thresholds, with either visual or electromyography (EMG) detection, to establish an intraoperative tool devoted to ensure safe distance of the electrode to the CSBT.
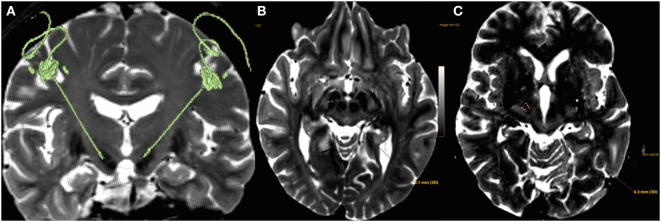
Twelve PD patients with subthalamic nucleus DBS participated. Thresholds of muscular contractions were assessed clinically and with EMG, for three different sets of stimulation parameters, all monopolar: 130 Hz high-frequency stimulation (HFS); 2 Hz low-frequency stimulation with either 60 or 210 µs (LFS-60, LFS-210). The anatomical distance of electrode contacts to CSBT was measured from fused CT-MRI.
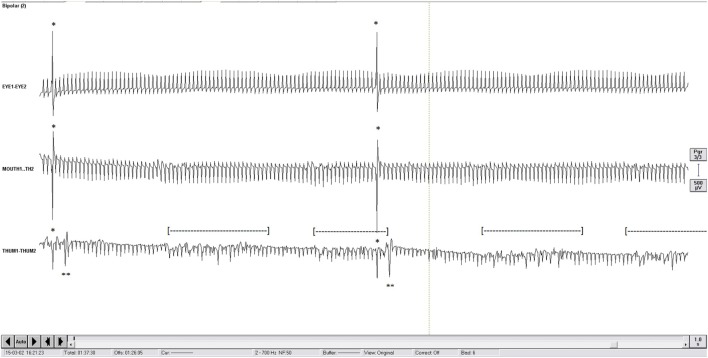
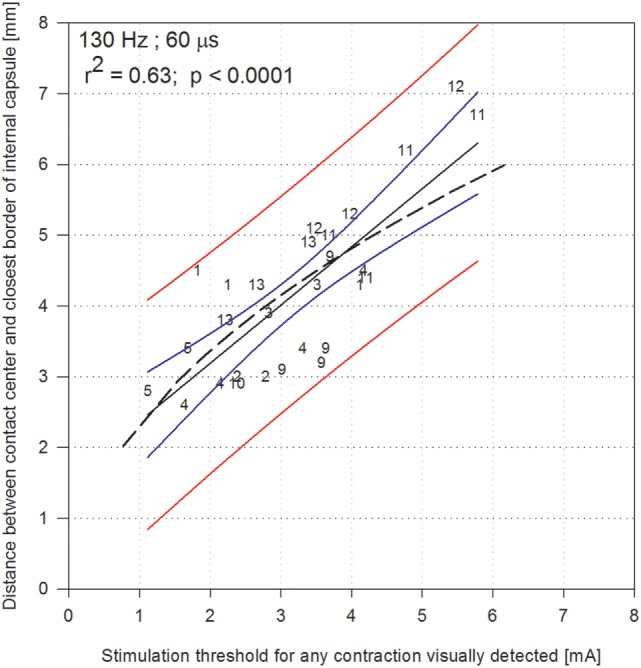
The best linear correlation was found for thresholds of visually detected contractions with HFS ( = 0.63, < 0.0001) when estimated stimulation currents rather than voltages were used. This correlation was found in agreement with an accepted model of electrical spatial extent of activation ( = 0.50). When using LFS, the correlation found remained lower than for HFS but increased when EMG was used. Indeed, the detection of contraction thresholds with EMG versus visual inspection did allow more frequent detection of face contractions, contributing to improve that correlation.
The correlation between electrode distance to the CSBT and contraction thresholds was found better when estimated with currents rather than voltage, eliminating the variance due to electrode impedance. Using LFS did not improve the precision of that evaluation, but EMG did. This technique provides a prediction band to ensure minimum distance of the electrode contacts to the CSBT, integrating the variance that can be encountered between prediction of models and practice.
帕金森病(PD)中成功的脑深部电刺激(DBS)需要最佳的电极放置。术中电极测试的一种技术是确定诱发皮质脊髓/皮质延髓束(CSBT)运动收缩的刺激阈值。
本研究旨在分析DBS电极与CSBT的距离和收缩阈值之间的相关性,采用视觉或肌电图(EMG)检测,以建立一种术中工具,致力于确保电极与CSBT的安全距离。
12例接受丘脑底核DBS的PD患者参与研究。针对三组不同的刺激参数(均为单极)评估肌肉收缩阈值,包括:130Hz高频刺激(HFS);2Hz低频刺激,脉宽分别为60或210µs(LFS - 60、LFS - 210)。通过融合的CT - MRI测量电极触点与CSBT的解剖距离。
当使用估计的刺激电流而非电压时,视觉检测到的收缩阈值与HFS之间的线性相关性最佳(r = 0.63,p < 0.0001)。这种相关性与公认的激活电空间范围模型一致(r = 0.50)。使用LFS时,发现的相关性仍低于HFS,但使用EMG时相关性增加。实际上,与视觉检查相比,EMG检测收缩阈值确实能更频繁地检测到面部收缩,有助于提高这种相关性。
当用电流而非电压估计时,发现电极与CSBT的距离和收缩阈值之间的相关性更好,消除了由于电极阻抗引起的差异。使用LFS并未提高该评估的精度,但EMG提高了精度。该技术提供了一个预测区间,以确保电极触点与CSBT的最小距离,整合了模型预测与实际应用之间可能出现的差异。