Cao Bochen, Bray Freddie, Beltrán-Sánchez Hiram, Ginsburg Ophira, Soneji Samir, Soerjomataram Isabelle
Section of Cancer Surveillance, International Agency for Research on Cancer, 69372 Lyon CEDEX 08, France
Section of Cancer Surveillance, International Agency for Research on Cancer, 69372 Lyon CEDEX 08, France.
BMJ. 2017 Jun 21;357:j2765. doi: 10.1136/bmj.j2765.
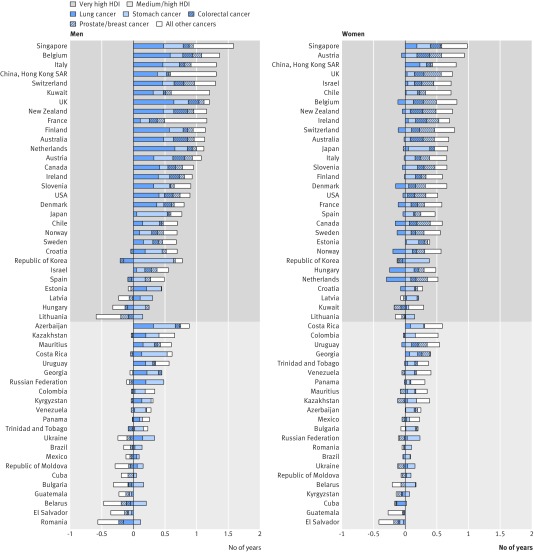
To quantify the impact of cancer (all cancers combined and major sites) compared with cardiovascular disease (CVD) on longevity worldwide during 1981-2010. Retrospective demographic analysis using aggregated data. National civil registration systems in member states of the World Health Organization. 52 populations with moderate to high quality data on cause specific mortality. Disease specific contributions to changes in life expectancy in ages 40-84 (LE) over time in populations grouped by two levels of Human Development Index (HDI) values. Declining CVD mortality rates during 1981-2010 contributed to, on average, over half of the gains in LE; the corresponding gains were 2.3 (men) and 1.7 (women) years, and 0.5 (men) and 0.8 (women) years in very high and medium and high HDI populations, respectively. Declines in cancer mortality rates contributed to, on average, 20% of the gains in LE or 0.8 (men) and 0.5 (women) years in very high HDI populations, and to over 10% or 0.2 years (both sexes) in medium and high HDI populations. Declining lung cancer mortality rates brought about the largest LE gain in men in very high HDI populations (up to 0.7 years in the Netherlands), whereas in medium and high HDI populations its contribution was smaller yet still positive. Among women, declines in breast cancer mortality rates were largely responsible for the improvement in longevity, particularly among very high HDI populations (up to 0.3 years in the United Kingdom). In contrast, losses in LE were observed in many medium and high HDI populations as a result of increasing breast cancer mortality rates. The control of CVD has led to substantial gains in LE worldwide. The inequality in improvement in longevity attributed to declining cancer mortality rates reflects inequities in implementation of cancer control, particularly in less resourced populations and in women. Global actions are needed to revitalize efforts for cancer control, with a specific focus on less resourced countries.
为了量化1981 - 2010年期间癌症(所有癌症综合及主要部位)与心血管疾病(CVD)对全球寿命的影响。使用汇总数据进行回顾性人口统计学分析。世界卫生组织成员国的国家民事登记系统。52个具有中高质量特定病因死亡率数据的人群。按人类发展指数(HDI)值的两个水平分组的人群中,特定疾病对40 - 84岁人群预期寿命(LE)随时间变化的贡献。1981 - 2010年期间CVD死亡率的下降平均促成了LE增长的一半以上;在极高和中高HDI人群中,相应的增长分别为男性2.3年和女性1.7年,以及男性0.5年和女性0.8年。癌症死亡率的下降平均促成了极高HDI人群中LE增长的20%或男性0.8年和女性0.5年,以及中高HDI人群中超过10%或两性均为0.2年的增长。肺癌死亡率的下降在极高HDI人群中的男性中带来了最大LE增长(荷兰高达0.7年),而在中高HDI人群中其贡献较小但仍为正向。在女性中,乳腺癌死亡率的下降在很大程度上促成了寿命的改善,特别是在极高HDI人群中(英国高达0.3年)。相比之下,由于乳腺癌死亡率上升,在许多中高HDI人群中观察到LE有所损失。CVD的控制在全球范围内带来了LE的大幅增长。归因于癌症死亡率下降的寿命改善不平等反映了癌症控制实施中的不公平,特别是在资源较少的人群和女性中。需要采取全球行动来重振癌症控制努力,特别关注资源较少的国家。