McAleese Kirsty E, Walker Lauren, Graham Sophie, Moya Elisa L J, Johnson Mary, Erskine Daniel, Colloby Sean J, Dey Madhurima, Martin-Ruiz Carmen, Taylor John-Paul, Thomas Alan J, McKeith Ian G, De Carli Charles, Attems Johannes
Institute of Neuroscience, Campus for Ageing and Vitality, Newcastle University, Newcastle upon Tyne, NE4 5PL, UK.
Department of Biology, University of Granada, Granada, Spain.
Acta Neuropathol. 2017 Sep;134(3):459-473. doi: 10.1007/s00401-017-1738-2. Epub 2017 Jun 21.
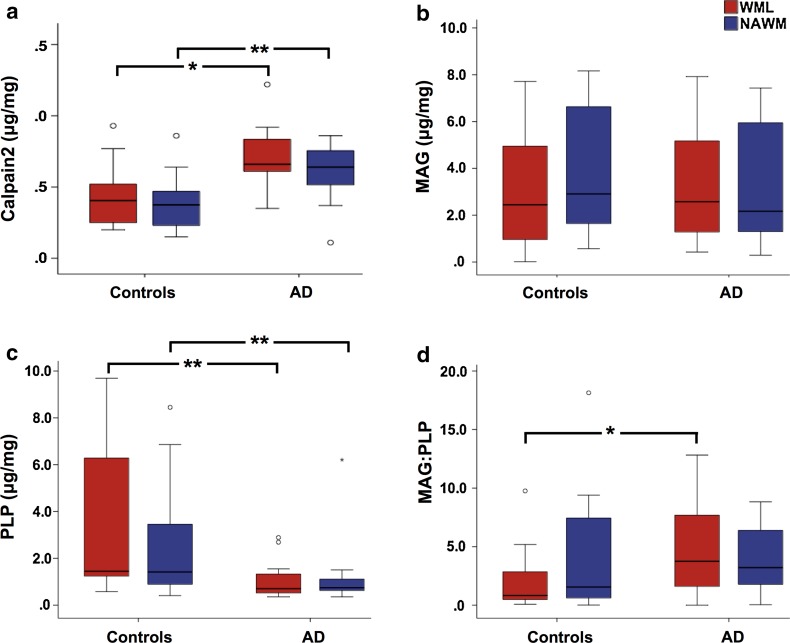
Cerebral white matter lesions (WML) encompass axonal loss and demyelination, and the pathogenesis is assumed to be small vessel disease (SVD)-related ischemia. However, WML may also result from the activation of Wallerian degeneration as a consequence of cortical Alzheimer's disease (AD) pathology, i.e. hyperphosphorylated tau (HPτ) and amyloid-beta (Aβ) deposition. WML seen in AD have a posterior predominance compared to non-demented individuals but it is unclear whether the pathological and molecular signatures of WML differ between these two groups. We investigated differences in the composition and aetiology of parietal WML from AD and non-demented controls. Parietal WML tissue from 55 human post-mortem brains (AD, n = 27; non-demented controls, n = 28) were quantitatively assessed for axonal loss and demyelination, as well as for cortical HPτ and Aβ burden and SVD. Biochemical assessment included Wallerian degeneration protease calpain and the myelin-associated glycoprotein (MAG) to proteolipid protein (PLP) ratio (MAG:PLP) as a measure of hypoperfusion. WML severity was associated with both axonal loss and demyelination in AD, but only with demyelination in controls. Calpain was significantly increased in WML tissue in AD, whereas MAG:PLP was significantly reduced in controls. Calpain levels were associated with increasing amounts of cortical AD-pathology but not SVD. We conclude that parietal WML seen in AD differ in their pathological composition and aetiology compared to WML seen in aged controls: WML seen in AD may be associated with Wallerian degeneration that is triggered by cortical AD-pathology, whereas WML in aged controls are due to ischaemia. Hence, parietal WML as seen on MRI should not invariably be interpreted as a surrogate biomarker for SVD as they may be indicative of cortical AD-pathology, and therefore, AD should also be considered as the main underlying cause for cognitive impairment in cases with parietal WML.
脑白质病变(WML)包括轴突丢失和脱髓鞘,其发病机制被认为与小血管疾病(SVD)相关的缺血有关。然而,WML也可能是由于皮质阿尔茨海默病(AD)病理改变导致的华勒氏变性激活所致,即过度磷酸化的tau蛋白(HPτ)和β淀粉样蛋白(Aβ)沉积。与非痴呆个体相比,AD患者的WML在后部更为常见,但尚不清楚这两组患者WML的病理和分子特征是否存在差异。我们研究了AD患者和非痴呆对照者顶叶WML在组成和病因方面的差异。对55例人类尸检大脑(AD组,n = 27;非痴呆对照组,n = 28)的顶叶WML组织进行了轴突丢失和脱髓鞘的定量评估,以及皮质HPτ、Aβ负荷和SVD的评估。生化评估包括华勒氏变性蛋白酶钙蛋白酶和髓鞘相关糖蛋白(MAG)与蛋白脂蛋白(PLP)的比值(MAG:PLP),作为灌注不足的指标。WML严重程度在AD患者中与轴突丢失和脱髓鞘均相关,但在对照组中仅与脱髓鞘相关。AD患者WML组织中的钙蛋白酶显著增加,而对照组中的MAG:PLP显著降低。钙蛋白酶水平与皮质AD病理改变的增加有关,但与SVD无关。我们得出结论,与老年对照组的WML相比,AD患者的顶叶WML在病理组成和病因方面存在差异:AD患者的WML可能与由皮质AD病理改变引发的华勒氏变性有关,而老年对照组的WML则是由于缺血所致。因此,MRI上所见的顶叶WML不应总是被解释为SVD的替代生物标志物,因为它们可能提示皮质AD病理改变,因此,在顶叶WML病例中,AD也应被视为认知障碍的主要潜在原因。