Abernethy Amy P, Arunachalam Ashwini, Burke Thomas, McKay Caroline, Cao Xiting, Sorg Rachael, Carbone David P
Flatiron Health, Inc., New York, New York, United States of America.
Duke University School of Medicine, Durham, North Carolina, United States of America.
PLoS One. 2017 Jun 23;12(6):e0178420. doi: 10.1371/journal.pone.0178420. eCollection 2017.
To establish a baseline for care and overall survival (OS) based upon contemporary first-line treatments prescribed in the era before the introduction of immune checkpoint inhibitors, for people with metastatic non-small cell lung cancer (NSCLC) without common actionable mutations.
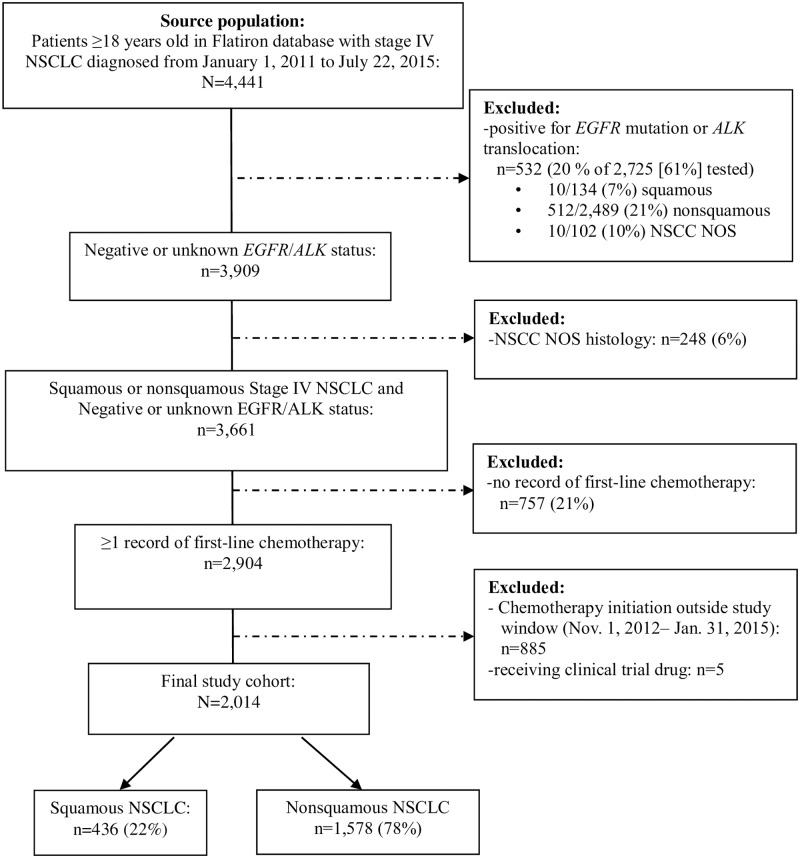
Using a nationally representative electronic health record data from the Flatiron dataset which included 162 practices from different regions in US, we identified patients (≥18 years old) newly diagnosed with stage IV NSCLC initiating first-line anticancer therapy (November 2012- January 2015, with follow-up through July 2015). Patients with documented epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) translocation were excluded. Anti-cancer drug therapy and overall survival were described overall, and by histology.
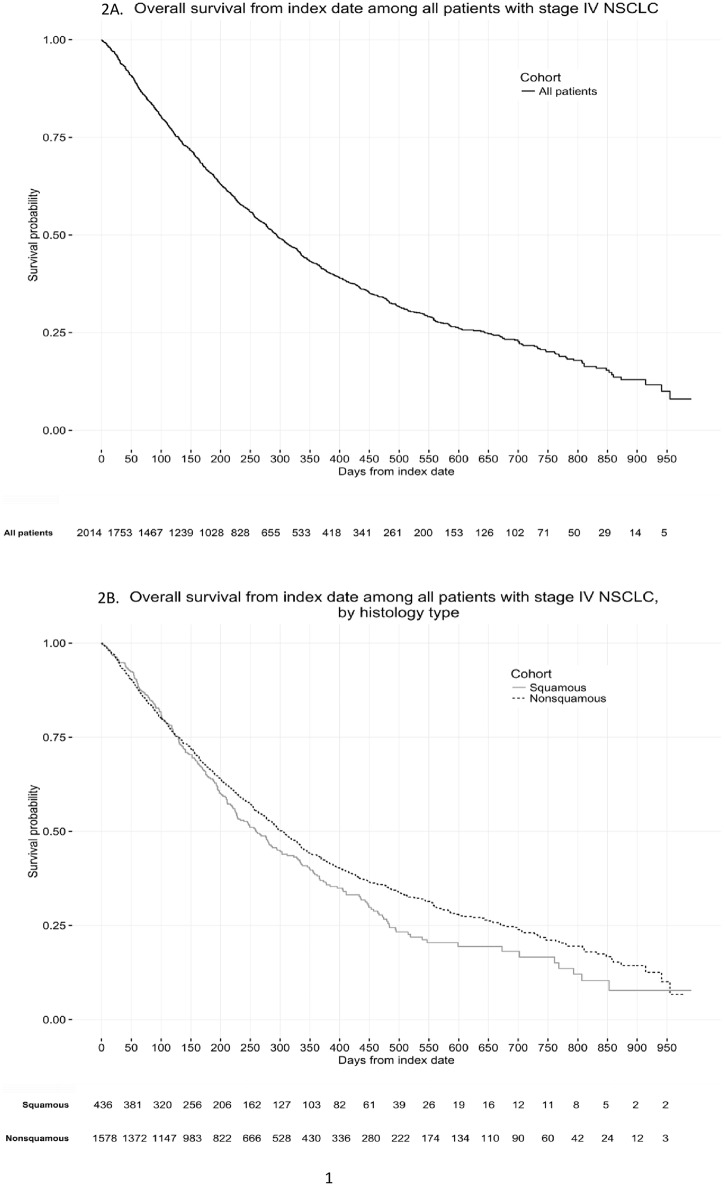
A total of 2,014 patients with stage IV NSCLC without known EGFR or ALK genomic tumor aberrations initiated systemic anticancer therapy, 22% with squamous and 78% with nonsquamous histology. Their mean (SD) age was 67 (10) years, 55% were male, and 87% had a smoking history. In nonsquamous NSCLC, carboplatin plus pemetrexed either without (25.7%) or with bevacizumab (16%) were the most common regimens; 26.6% of nonsquamous patients receiving induction therapy also received continuation maintenance therapy. In squamous NSCLC, carboplatin plus paclitaxel (37.6%) or nab-paclitaxel (21.1%) were the most commonly used regimens. Overall median OS was 9.7 months (95% CI: 9.1, 10.3), 8.5 months (95% CI: 7.4, 10.0) for squamous, and 10.0 months (95% CI: 9.4, 10.8) for nonsquamous NSCLC.
The results provide context for evaluating the effect of shifting treatment patterns of NSCLC treatments on patient outcomes, and for community oncology benchmarking initiatives.
为无常见可操作突变的转移性非小细胞肺癌(NSCLC)患者,建立基于免疫检查点抑制剂引入之前时代所规定的当代一线治疗的护理和总生存期(OS)基线。
使用来自Flatiron数据集的具有全国代表性的电子健康记录数据,该数据集包括美国不同地区的162家医疗机构,我们确定了新诊断为IV期NSCLC并开始一线抗癌治疗的患者(≥18岁)(2012年11月至2015年1月,随访至2015年7月)。记录有表皮生长因子受体(EGFR)或间变性淋巴瘤激酶(ALK)易位的患者被排除。总体描述了抗癌药物治疗和总生存期,并按组织学进行了描述。
共有2014例无已知EGFR或ALK基因组肿瘤畸变的IV期NSCLC患者开始全身抗癌治疗,22%为鳞状组织学,78%为非鳞状组织学。他们的平均(标准差)年龄为67(10)岁,55%为男性,87%有吸烟史。在非鳞状NSCLC中,最常见的方案是卡铂加培美曲塞(无贝伐单抗时为25.7%,加贝伐单抗时为16%);26.6%接受诱导治疗的非鳞状患者也接受了持续维持治疗。在鳞状NSCLC中,最常用的方案是卡铂加紫杉醇(37.6%)或白蛋白结合型紫杉醇(21.1%)。总体中位OS为9.7个月(95%CI:9.1,10.3),鳞状NSCLC为8.5个月(95%CI:7.4,10.0),非鳞状NSCLC为10.0个月(95%CI:9.4,10.8)。
这些结果为评估NSCLC治疗模式转变对患者预后的影响以及社区肿瘤学基准计划提供了背景。