Department of Thoracic Oncology, Thoraxklinik at the University of Heidelberg, 69126 Heidelberg, Germany.
Respir Res. 2013 Dec 18;14(1):139. doi: 10.1186/1465-9921-14-139.
Most patients with metastatic non-small cell lung cancer (NSCLC) will face treatment with systemic therapy. Current clinical studies are demonstrating improvements in chemotherapy and overall survival. However, it remains unclear whether these results are translated into clinical practice.
We reviewed all stage IV NSCLC patients without second malignancies that were diagnosed from 2004 to 2006 at our institution. 493 consecutive patients were included into this retrospective analysis and were followed-up until end of 2011.
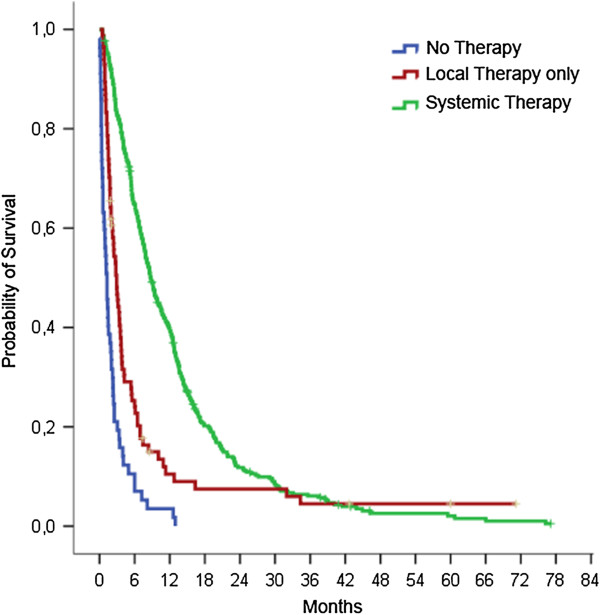
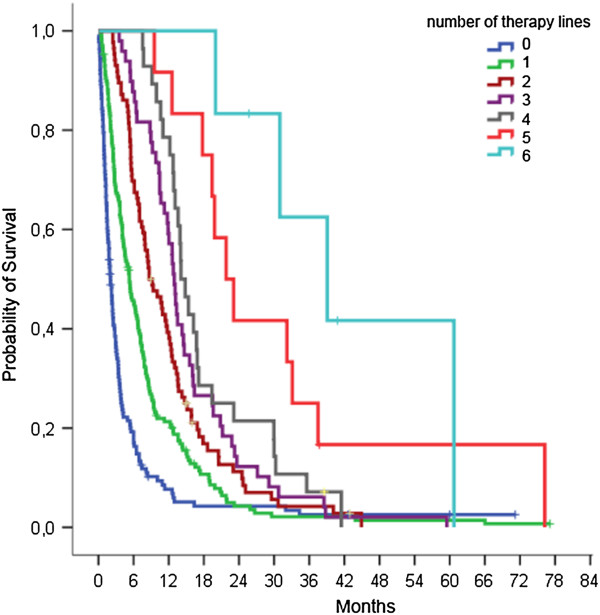
352 patients (71.4%) received systemic therapy for up to 7 lines. For most patients, adjustments of dosages or applications had to be made at some point of the treatment, but the total applied dose remained generally close to the intended dose. The best disease control (BDC) rate decreased with increasing therapy lines from 59.7% to about 35%. Patients with palliative local therapy but no systemic treatment demonstrated inferior survival (median 2.9 versus 8.7 months, p < 0.001). The median interval between last treatment and death was 50 days and 15 days for chemotherapy and anti-EGFR therapy, respectively. BDC to the previous therapy lines was predictive for improved BDC to third- but not second-line therapy. Performing multivariate analysis, BDC to previous therapy, never-/ former-smoking status, and age > 70 years were associated with improved survival performing third-line therapy.
Stage IV NSCLC patients may receive substantial systemic therapy resulting in response and median survival rates that are comparable to data from clinical studies. However, preselection factors are increasingly important to improve therapy outcome and life quality.
大多数转移性非小细胞肺癌(NSCLC)患者将面临系统治疗。目前的临床研究表明化疗和总生存期有所改善。然而,这些结果是否转化为临床实践尚不清楚。
我们回顾了我院 2004 年至 2006 年期间诊断的所有无第二恶性肿瘤的 IV 期 NSCLC 患者。共有 493 例连续患者纳入本回顾性分析,并随访至 2011 年底。
352 例(71.4%)患者接受了多达 7 线的系统治疗。对于大多数患者,在治疗过程中必须调整剂量或应用,但总应用剂量通常接近预期剂量。最佳疾病控制(BDC)率随着治疗线数的增加从 59.7%降至约 35%。有姑息性局部治疗但无全身治疗的患者生存较差(中位 2.9 个月与 8.7 个月,p<0.001)。末次治疗与死亡之间的中位间隔时间分别为化疗和抗 EGFR 治疗的 50 天和 15 天。前一线治疗的 BDC 可预测三线治疗的 BDC 改善,但不能预测二线治疗的 BDC 改善。进行多变量分析,前一线治疗的 BDC、从不/曾经吸烟状态和年龄>70 岁与三线治疗的生存改善相关。
IV 期 NSCLC 患者可能接受大量的系统治疗,导致反应和中位生存时间与临床研究数据相当。然而,筛选因素对于提高治疗效果和生活质量越来越重要。