Mack Ines, Burckhardt Marie-Anne, Heininger Ulrich, Prüfer Friederike, Schulzke Sven, Wellmann Sven
Pediatric Infectious Diseases, University of Basel Children's Hospital (UKBB), Basel, Switzerland.
Department of Endocrinology and Diabetes, Princess Margaret Hospital for Children, Perth, WA, Australia.
Front Pediatr. 2017 Jun 9;5:134. doi: 10.3389/fped.2017.00134. eCollection 2017.
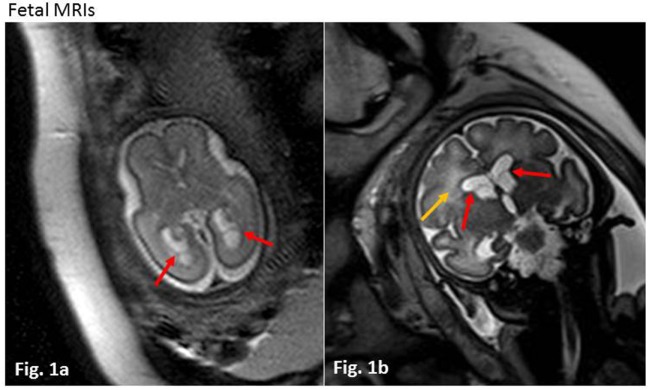
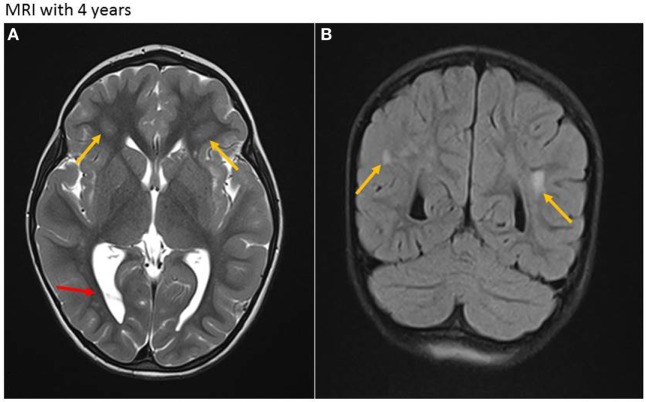
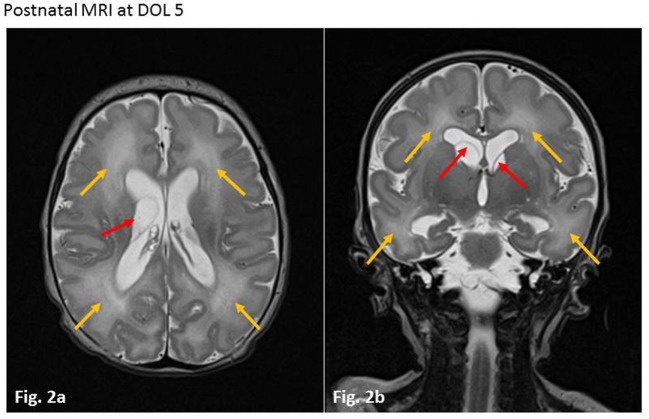
Cytomegalovirus (CMV) is the most frequent congenital virus infection worldwide. The risk of congenital CMV (cCMV) transmission is highest in seronegative women who acquire primary CMV infection during pregnancy. A growing body of evidence indicates that secondary CMV infections in pregnant women with preconceptual immunity (either through reactivation of latent virus or re-infection with a new strain of CMV) contribute to a much greater proportion of symptomatic cCMV than was previously thought. Here, we describe a case of symptomatic cCMV infection in the newborn of a woman with proven immunity prior to pregnancy. Diagnosis was confirmed by CMV PCR from amniotic fluid and fetal MR imaging. The newborn presented with typical cCMV symptoms including jaundice, hepatosplenomegaly, cholestasis, petechiae, small head circumference, and sensorineural hearing loss, the most common neurologic sequela. CMV was detected in infant blood and urine by PCR, and intravenous ganciclovir was initiated and continued orally for 6 weeks totally. Apart from persisting right-sided deafness, the child exhibited normal neurological development up through the last follow-up at 4.5 years. To date, the most effective strategy to prevent vertical CMV transmission is hygiene counseling for women of childbearing age, which, in our case, and in concordance with recent literature, applies to seronegative, as well as seropositive, women. Once an expecting mother shows seroconversion or signs of an active CMV infection, there are no established procedures to reduce the risk of transmission, or therapeutic options for the fetus with signs of infection. After birth, symptomatic infants can be treated with ganciclovir to inhibit viral replication and improve hearing ability and neurodevelopmental outcome. A comprehensive review of the literature, including our case study, reveals the most current and significant diagnostic and treatment options available. In conclusion, the triad of maternal hygiene counseling, postnatal hearing screening of all newborns, followed by CMV PCR in symptomatic infants, and antiviral therapy of infants with symptomatic cCMV provides an outline of best practice to reduce the burden of CMV transmission sequelae.
巨细胞病毒(CMV)是全球最常见的先天性病毒感染。先天性CMV(cCMV)传播风险在孕期发生原发性CMV感染的血清阴性女性中最高。越来越多的证据表明,孕前具有免疫力的孕妇发生继发性CMV感染(无论是潜伏病毒重新激活还是感染新的CMV毒株)导致有症状的cCMV的比例比之前认为的要高得多。在此,我们描述一例有症状的cCMV感染病例,该病例发生在一名孕前已证实具有免疫力的女性的新生儿身上。通过羊水CMV PCR检测和胎儿磁共振成像确诊。新生儿出现典型的cCMV症状,包括黄疸、肝脾肿大、胆汁淤积、瘀点、小头围和感音神经性听力损失,这是最常见的神经后遗症。通过PCR在婴儿血液和尿液中检测到CMV,并开始静脉注射更昔洛韦,随后口服持续6周。除了持续存在的右侧耳聋外,该儿童在4.5岁的最后一次随访时神经发育正常。迄今为止,预防CMV垂直传播的最有效策略是对育龄妇女进行卫生咨询,在我们的病例中,与最近的文献一致,这适用于血清阴性以及血清阳性的女性。一旦孕妇出现血清转化或活动性CMV感染的迹象,目前尚无既定程序来降低传播风险,也没有针对有感染迹象胎儿的治疗选择。出生后,有症状的婴儿可用更昔洛韦治疗以抑制病毒复制并改善听力和神经发育结局。对包括我们的病例研究在内的文献进行全面综述,揭示了当前可用的最新且重要的诊断和治疗选择。总之,孕产妇卫生咨询、对所有新生儿进行产后听力筛查,随后对有症状婴儿进行CMV PCR检测,以及对有症状的cCMV婴儿进行抗病毒治疗,这三者构成了减轻CMV传播后遗症负担的最佳实践概述。