Mühlberger Nikolai, Boskovic Kristijan, Krahn Murray D, Bremner Karen E, Oberaigner Willi, Klocker Helmut, Horninger Wolfgang, Sroczynski Gaby, Siebert Uwe
Institute of Public Health, Medical Decision Making and Health Technology Assessment, Department of Public Health, Health Services Research and Health Technology Assessment, UMIT - University for Health Sciences, Medical Informatics and Technology, Eduard-Wallnoefer-Zentrum 1, A-6060, Hall i.T, Austria.
Division of Health Technology Assessment, ONCOTYROL - Center for Personalized Cancer Medicine, Innsbruck, Austria.
BMC Public Health. 2017 Jun 26;17(1):596. doi: 10.1186/s12889-017-4439-9.
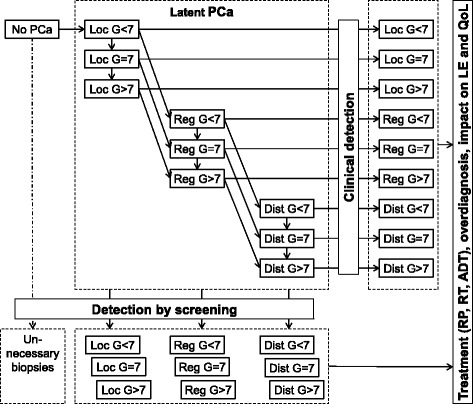
A recent recalibration of the ONCOTYROL Prostate Cancer Outcome and Policy (PCOP) Model, assuming that latent prostate cancer (PCa) detectable at autopsy might be detectable by screening as well, resulted in considerable worsening of the benefit-harm balance of screening. In this study, we used the recalibrated model to assess the effects of familial risk, quality of life (QoL) preferences, age, and active surveillance.
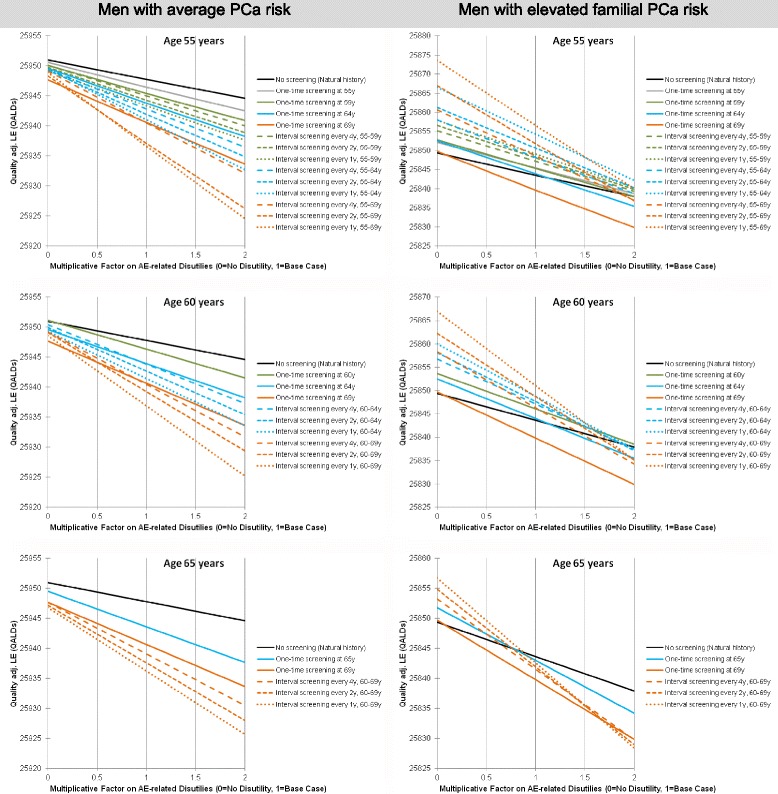
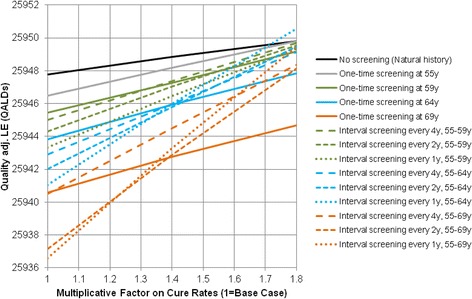
Men with average and elevated familial PCa risk were simulated in separate models, differing in familial risk parameters. Familial risk was assumed to affect PCa onset and progression simultaneously in the base-case, and separately in scenario analyses. Evaluated screening strategies included one-time screening at different ages, and screening at different intervals and age ranges. Optimal screening strategies were identified depending on age and individual QoL preferences. Strategies were additionally evaluated with active surveillance by biennial re-biopsy delaying treatment of localized cancer until grade progression to Gleason score ≥ 7.
Screening men with average PCa risk reduced quality-adjusted life expectancy (QALE) even under favorable assumptions. Men with elevated familial risk, depending on age and disutilities, gained QALE. While for men with familial risk aged 55 and 60 years annual screening to age 69 was the optimal strategy over most disutility ranges, no screening was the preferred option for 65 year-old men with average and above disutilities. Active surveillance greatly reduced overtreatment, but QALE gains by averted adverse events were opposed by losses due to delayed treatment and additional biopsies. The effect of active surveillance on the benefit-harm balance of screening differed between populations, as net losses and gains in QALE predicted for screening without active surveillance in men with average and familial PCa risk, respectively, were both reduced.
Assumptions about PCa risk and screen-detectable prevalence significantly affect the benefit-harm balance of screening. Based on the assumptions of our model, PCa screening should focus on candidates with familial predisposition with consideration of individual QoL preferences and age. Active surveillance may require treatment initiation before Gleason score progression to 7. Alternative active surveillance strategies should be evaluated in further modeling studies.
最近对ONCOTYROL前列腺癌结局与政策(PCOP)模型进行了重新校准,假设尸检时可检测到的潜伏性前列腺癌(PCa)也可能通过筛查检测到,这导致筛查的利弊平衡显著恶化。在本研究中,我们使用重新校准的模型来评估家族风险、生活质量(QoL)偏好、年龄和主动监测的影响。
在不同家族风险参数的单独模型中模拟平均家族性PCa风险和高家族性PCa风险的男性。在基础病例中,假设家族风险同时影响PCa的发病和进展,在情景分析中则分别影响。评估的筛查策略包括在不同年龄进行一次性筛查,以及在不同间隔和年龄范围进行筛查。根据年龄和个体QoL偏好确定最佳筛查策略。通过每两年重新活检进行主动监测,将局限性癌症的治疗推迟到Gleason评分进展至≥7级,对策略进行了额外评估。
即使在有利的假设下,对平均PCa风险的男性进行筛查也会降低质量调整生命预期(QALE)。高家族风险的男性根据年龄和负效用获得了QALE。对于55岁和60岁的家族风险男性,在大多数负效用范围内,至69岁每年进行筛查是最佳策略,而对于65岁平均及以上负效用的男性,不进行筛查是首选方案。主动监测大大减少了过度治疗,但避免不良事件带来的QALE增加被延迟治疗和额外活检造成的损失所抵消。主动监测对筛查利弊平衡的影响在不同人群中有所不同,因为在平均PCa风险和家族性PCa风险男性中,预测的无主动监测筛查的QALE净损失和净收益均有所减少。
关于PCa风险和筛查可检测患病率的假设显著影响筛查的利弊平衡。基于我们模型的假设,PCa筛查应关注有家族易感性的人群,并考虑个体QoL偏好和年龄。主动监测可能需要在Gleason评分进展至7级之前开始治疗。应在进一步的建模研究中评估替代的主动监测策略。