Davis Katherine Finn, Napolitano Natalie, Li Simon, Buffman Hayley, Rehder Kyle, Pinto Matthew, Nett Sholeen, Jarvis J Dean, Kamat Pradip, Sanders Ronald C, Turner David A, Sullivan Janice E, Bysani Kris, Lee Anthony, Parker Margaret, Adu-Darko Michelle, Giuliano John, Biagas Katherine, Nadkarni Vinay, Nishisaki Akira
1University of Hawai'i at Mānoa, School of Nursing and Dental Hygiene, Honolulu, HI. 2Department of Respiratory Therapy, Children's Hospital of Philadelphia, Philadelphia, PA. 3Division of Pediatric Critical Care Medicine, Department of Pediatrics, Maria Fareri Children's Hospital, Valhalla, NY. 4Department of Pediatrics, New York Medical College, Valhalla, NY. 5Center for Simulation, Advanced Education and Innovation, Children's Hospital of Philadelphia, Philadelphia, PA. 6Department of Pediatrics, Division of Critical Care, Duke Children's Hospital, Durham, NC. 7Department of Pediatrics, Dartmouth-Hitchcock Medical Center, Lebanon, NH. 8Department of Pediatrics, Emory University School of Medicine, Children's Hospital of Atlanta, Atlanta, GA. 9Department of Pediatrics, Section of Pediatric Critical Care, UAMS/Arkansas Children's Hospital, Little Rock, AR. 10Department of Pediatrics, Division of Critical Care, University of Louisville and Norton Children's Hospital, Louisville, KY. 11Pediatric Critical Care Medicine, Medical City Children's Hospital, Dallas, TX. 12Nationwide Children's Hospital, Columbus, OH. 13Department of Pediatrics, Pediatric Critical Care Medicine, Stony Brook Children's Hospital, Stony Brook, NY. 14Pediatric Critical Care Medicine, The University of Virginia Health System Children's Hospital, Charlottesville, VA. 15Yale Pediatric Critical Care Medicine, Yale-New Haven Children's Hospital, New Haven, CT. 16Department of Pediatrics, Columbia University Medical Center, New York, NY. 17Department of Anesthesiology and Critical Care Medicine, Children's Hospital of Philadelphia, Philadelphia, PA.
Pediatr Crit Care Med. 2017 Oct;18(10):965-972. doi: 10.1097/PCC.0000000000001251.
To describe promoters and barriers to implementation of an airway safety quality improvement bundle from the perspective of interdisciplinary frontline clinicians and ICU quality improvement leaders.
Mixed methods.
Thirteen PICUs of the National Emergency Airway Registry for Children network.
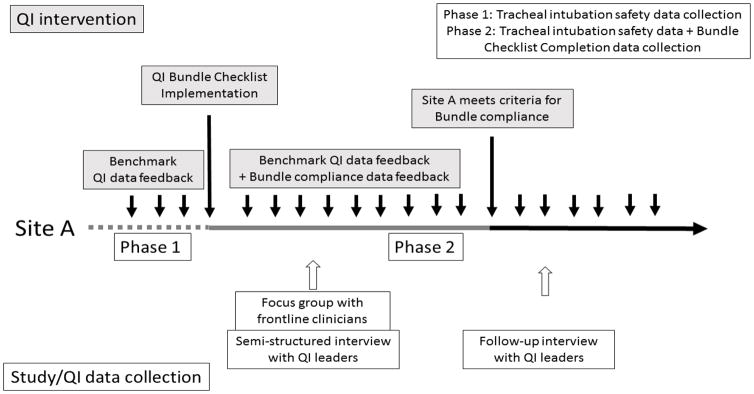
Remote or on-site focus groups with interdisciplinary ICU staff. Two semistructured interviews with ICU quality improvement leaders with quantitative and qualitative data-based feedbacks.
Bundle implementation success (compliance) was defined as greater than or equal to 80% use for tracheal intubations for 3 consecutive months. ICUs were classified as early or late adopters. Focus group discussions concentrated on safety concerns and promoters and barriers to bundle implementation. Initial semistructured quality improvement leader interviews assessed implementation tactics and provided recommendations. Follow-up interviews assessed degree of acceptance and changes made after initial interview. Transcripts were thematically analyzed and contrasted by early versus late adopters. Median duration to achieve success was 502 days (interquartile range, 182-781). Five sites were early (median, 153 d; interquartile range, 146-267) and eight sites were late adopters (median, 783 d; interquartile range, 773-845). Focus groups identified common "promoter" themes-interdisciplinary approach, influential champions, and quality improvement bundle customization-and "barrier" themes-time constraints, competing paperwork and quality improvement activities, and poor engagement. Semistructured interviews with quality improvement leaders identified effective and ineffective tactics implemented by early and late adopters. Effective tactics included interdisciplinary quality improvement team involvement (early adopter: 5/5, 100% vs late adopter: 3/8, 38%; p = 0.08); ineffective tactics included physician-only rollouts, lack of interdisciplinary education, lack of data feedback to frontline clinicians, and misconception of bundle as research instead of quality improvement intervention.
Implementation of an airway safety quality improvement bundle with high compliance takes a long time across diverse ICUs. Both early and late adopters identified similar promoter and barrier themes. Early adopter sites customized the quality improvement bundle and had an interdisciplinary quality improvement team approach.
从跨学科一线临床医生和重症监护病房(ICU)质量改进负责人的角度,描述气道安全质量改进综合措施的推广因素和实施障碍。
混合方法。
国家儿童紧急气道注册网络的13个儿科重症监护病房。
与跨学科ICU工作人员进行远程或现场焦点小组讨论。对ICU质量改进负责人进行两次半结构化访谈,并基于定量和定性数据提供反馈。
综合措施实施成功(合规)定义为连续3个月气管插管使用率大于或等于80%。ICU被分为早期采用者或晚期采用者。焦点小组讨论集中在安全问题以及综合措施实施的推广因素和障碍。最初的半结构化质量改进负责人访谈评估了实施策略并提供了建议。后续访谈评估了接受程度以及初次访谈后所做的改变。对访谈记录进行主题分析,并按早期和晚期采用者进行对比。实现成功的中位时间为502天(四分位间距,182 - 781天)。5个地点为早期采用者(中位时间,153天;四分位间距,146 - 267天),8个地点为晚期采用者(中位时间,783天;四分位间距,773 - 845天)。焦点小组确定了常见的“推广因素”主题——跨学科方法、有影响力的倡导者以及质量改进综合措施的定制——和“障碍”主题——时间限制、相互竞争的文书工作和质量改进活动以及参与度低。对质量改进负责人的半结构化访谈确定了早期和晚期采用者实施的有效和无效策略。有效策略包括跨学科质量改进团队的参与(早期采用者:5/5,100%;晚期采用者:3/8,38%;p = 0.08);无效策略包括仅由医生推行、缺乏跨学科教育、缺乏向一线临床医生的数据反馈以及将综合措施误解为研究而非质量改进干预。
在不同的ICU中,实施高合规性的气道安全质量改进综合措施需要很长时间。早期和晚期采用者都确定了类似的推广因素和障碍主题。早期采用者站点对质量改进综合措施进行了定制,并采用了跨学科质量改进团队的方法。