Lovell Karina, Bower Peter, Gellatly Judith, Byford Sarah, Bee Penny, McMillan Dean, Arundel Catherine, Gilbody Simon, Gega Lina, Hardy Gillian, Reynolds Shirley, Barkham Michael, Mottram Patricia, Lidbetter Nicola, Pedley Rebecca, Molle Jo, Peckham Emily, Knopp-Hoffer Jasmin, Price Owen, Connell Janice, Heslin Margaret, Foley Christopher, Plummer Faye, Roberts Christopher
Division of Nursing, Midwifery and Social Work, School of Health Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester, United Kingdom.
NIHR School for Primary Care Research, University of Manchester, Manchester, United Kingdom.
PLoS Med. 2017 Jun 27;14(6):e1002337. doi: 10.1371/journal.pmed.1002337. eCollection 2017 Jun.
Obsessive-compulsive disorder (OCD) is prevalent and without adequate treatment usually follows a chronic course. "High-intensity" cognitive-behaviour therapy (CBT) from a specialist therapist is current "best practice." However, access is difficult because of limited numbers of therapists and because of the disabling effects of OCD symptoms. There is a potential role for "low-intensity" interventions as part of a stepped care model. Low-intensity interventions (written or web-based materials with limited therapist support) can be provided remotely, which has the potential to increase access. However, current evidence concerning low-intensity interventions is insufficient. We aimed to determine the clinical effectiveness of 2 forms of low-intensity CBT prior to high-intensity CBT, in adults meeting the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for OCD.
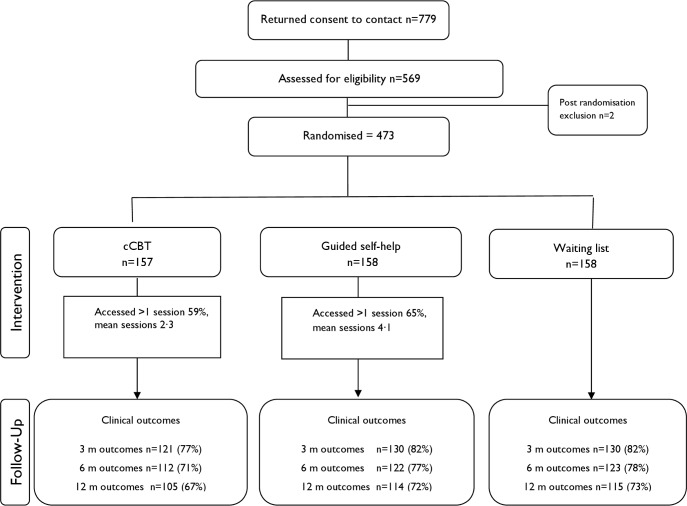
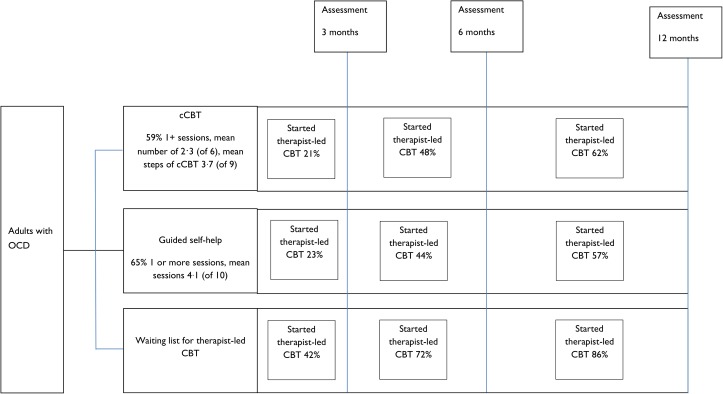
This study was approved by the National Research Ethics Service Committee North West-Lancaster (reference number 11/NW/0276). All participants provided informed consent to take part in the trial. We conducted a 3-arm, multicentre randomised controlled trial in primary- and secondary-care United Kingdom mental health services. All patients were on a waiting list for therapist-led CBT (treatment as usual). Four hundred and seventy-three eligible patients were recruited and randomised. Patients had a median age of 33 years, and 60% were female. The majority were experiencing severe OCD. Patients received 1 of 2 low-intensity interventions: computerised CBT (cCBT; web-based CBT materials and limited telephone support) through "OCFighter" or guided self-help (written CBT materials with limited telephone or face-to-face support). Primary comparisons concerned OCD symptoms, measured using the Yale-Brown Obsessive Compulsive Scale-Observer-Rated (Y-BOCS-OR) at 3, 6, and 12 months. Secondary outcomes included health-related quality of life, depression, anxiety, and functioning. At 3 months, guided self-help demonstrated modest benefits over the waiting list in reducing OCD symptoms (adjusted mean difference = -1.91, 95% CI -3.27 to -0.55). These effects did not reach a prespecified level of "clinically significant benefit." cCBT did not demonstrate significant benefit (adjusted mean difference = -0.71, 95% CI -2.12 to 0.70). At 12 months, neither guided self-help nor cCBT led to differences in OCD symptoms. Early access to low-intensity interventions led to significant reductions in uptake of high-intensity CBT over 12 months; 86% of the patients allocated to the waiting list for high-intensity CBT started treatment by the end of the trial, compared to 62% in supported cCBT and 57% in guided self-help. These reductions did not compromise longer-term patient outcomes. Data suggested small differences in satisfaction at 3 months, with patients more satisfied with guided self-help than supported cCBT. A significant issue in the interpretation of the results concerns the level of access to high-intensity CBT before the primary outcome assessment.
We have demonstrated that providing low-intensity interventions does not lead to clinically significant benefits but may reduce uptake of therapist-led CBT.
International Standard Randomized Controlled Trial Number (ISRCTN) Registry ISRCTN73535163.
强迫症(OCD)很常见,若未得到充分治疗,通常会呈慢性病程。由专科治疗师提供的“高强度”认知行为疗法(CBT)是目前的“最佳治疗方法”。然而,由于治疗师数量有限以及强迫症症状的致残影响,获得这种治疗存在困难。“低强度”干预作为阶梯式护理模式的一部分可能发挥作用。低强度干预(有有限治疗师支持的书面或基于网络的材料)可以远程提供,这有可能增加可及性。然而,目前关于低强度干预的证据不足。我们旨在确定在符合《精神疾病诊断与统计手册》第四版(DSM-IV)强迫症标准的成年人中,在进行高强度CBT之前,两种低强度CBT形式的临床疗效。
本研究获得了西北兰开夏郡国家研究伦理服务委员会的批准(参考编号11/NW/0276)。所有参与者均提供了参与试验的知情同意书。我们在英国初级和二级医疗心理健康服务机构中进行了一项三臂、多中心随机对照试验。所有患者都在等待由治疗师主导的CBT(常规治疗)。招募并随机分配了473名符合条件的患者。患者的中位年龄为33岁,60%为女性。大多数患者患有重度强迫症。患者接受以下两种低强度干预之一:通过“OCFighter”进行的计算机化CBT(cCBT;基于网络的CBT材料和有限的电话支持)或引导式自助(有有限电话或面对面支持的书面CBT材料)。主要比较涉及在3个月、6个月和12个月时使用耶鲁-布朗强迫症量表-观察者评定版(Y-BOCS-OR)测量的强迫症症状。次要结局包括与健康相关的生活质量、抑郁、焦虑和功能状况。在3个月时,引导式自助在减轻强迫症症状方面比等待名单组显示出适度益处(调整后平均差异=-1.91,95%置信区间-3.27至-0.55)。这些效果未达到预先设定的“临床显著益处”水平。cCBT未显示出显著益处(调整后平均差异=-0.71,95%置信区间-2.12至0.70)。在12个月时,引导式自助和cCBT均未导致强迫症症状出现差异。提前获得低强度干预导致12个月内高强度CBT的接受率显著降低;分配到高强度CBT等待名单组的患者中,86%在试验结束时开始治疗,而在有支持的cCBT组中为62%,引导式自助组中为57%。这些降低并未影响患者的长期结局。数据表明在3个月时满意度存在微小差异,患者对引导式自助的满意度高于有支持的cCBT。结果解释中的一个重要问题涉及主要结局评估之前获得高强度CBT的可及性水平。
我们已经证明,提供低强度干预不会带来临床显著益处,但可能会降低由治疗师主导的CBT的接受率。
国际标准随机对照试验编号(ISRCTN)注册库ISRCTN73535163 。