Szekely Eszter, Sudre Gustavo P, Sharp Wendy, Leibenluft Ellen, Shaw Philip
From the Section on Neurobehavioral and Clinical Research, Social and Behavioral Research Branch, National Human Genome Research Institute, Bethesda, Md.; and the Section on Bipolar Spectrum Disorders, Emotion and Development Branch, National Institute of Mental Health, Bethesda, Md.
Am J Psychiatry. 2017 Sep 1;174(9):867-876. doi: 10.1176/appi.ajp.2017.16111313. Epub 2017 Jun 29.
Understanding the neural processes tied to the adult outcome of childhood attention deficit hyperactivity disorder (ADHD) could guide novel interventions to improve its clinical course. It has been argued that normalization of prefrontal cortical activity drives remission from ADHD, while anomalies in subcortical processes are "fixed," present even in remission. Using multimodal neuroimaging of inhibitory processes, the authors tested these hypotheses in adults followed since childhood, contrasting remitted against persistent ADHD.
Adult participants (persistent ADHD, N=35; remit-ted ADHD, N=47; never affected, N=99) were scanned with functional MRI (fMRI) (N=85), magnetoencephalography (N=33), or both (N=63) during a response inhibition task.
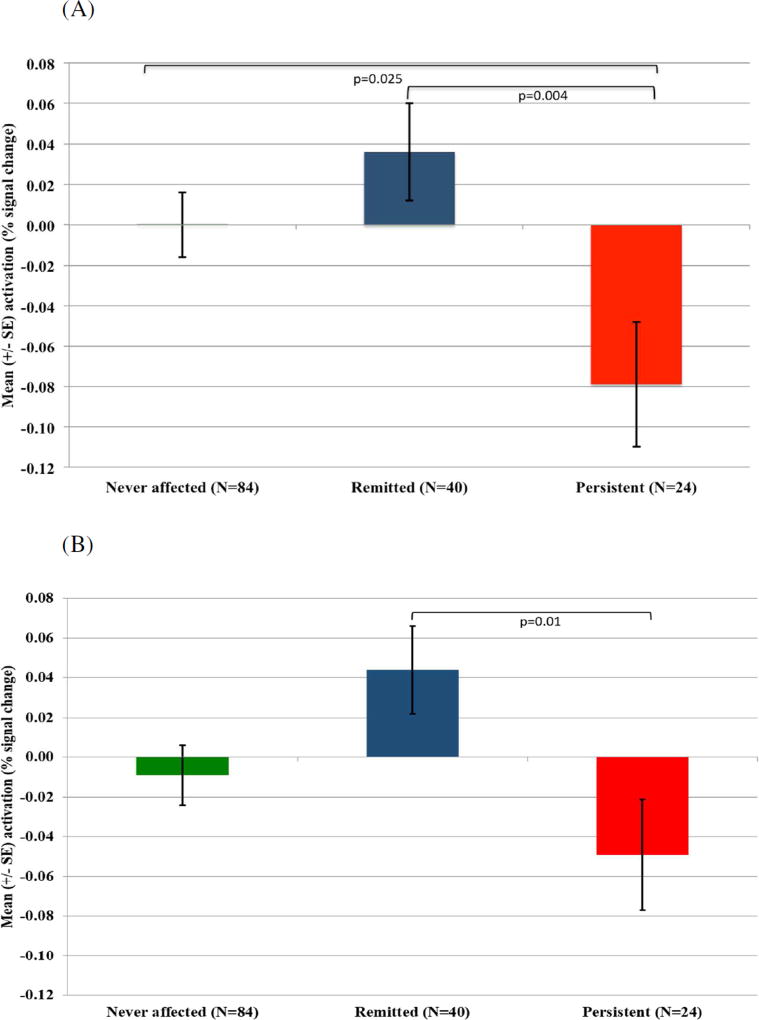
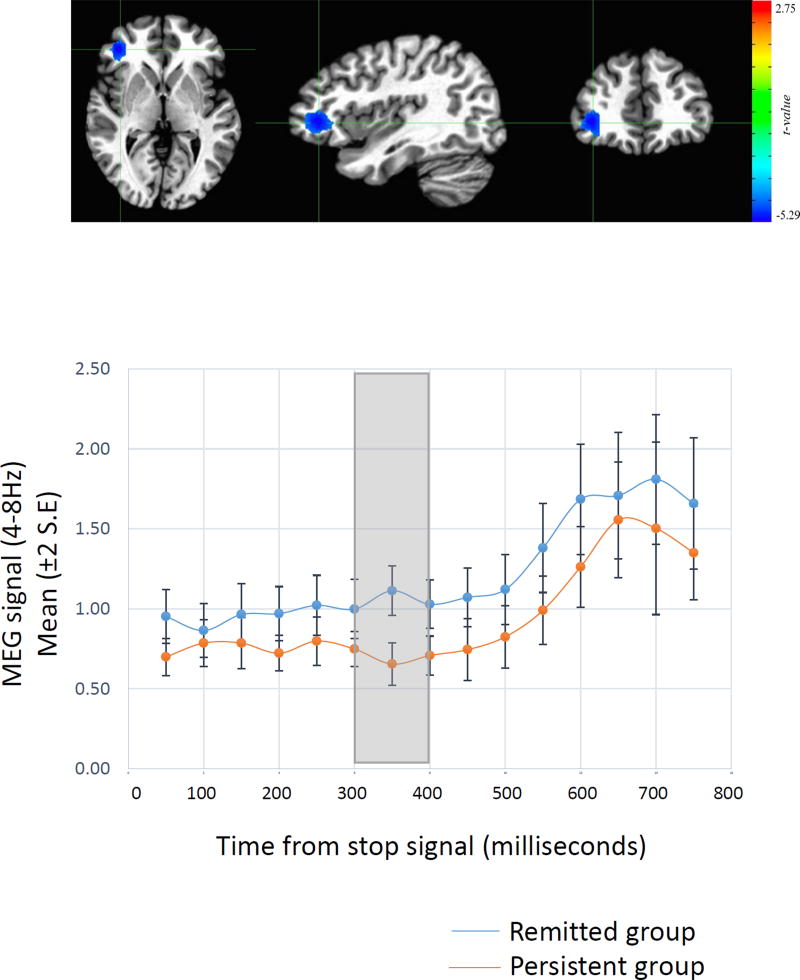
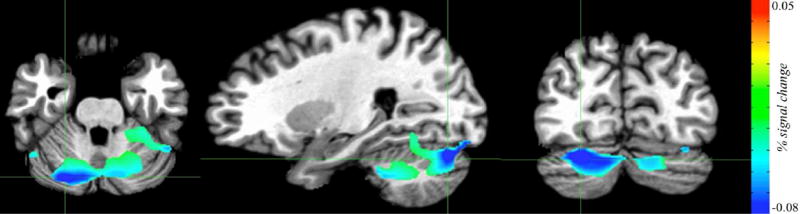
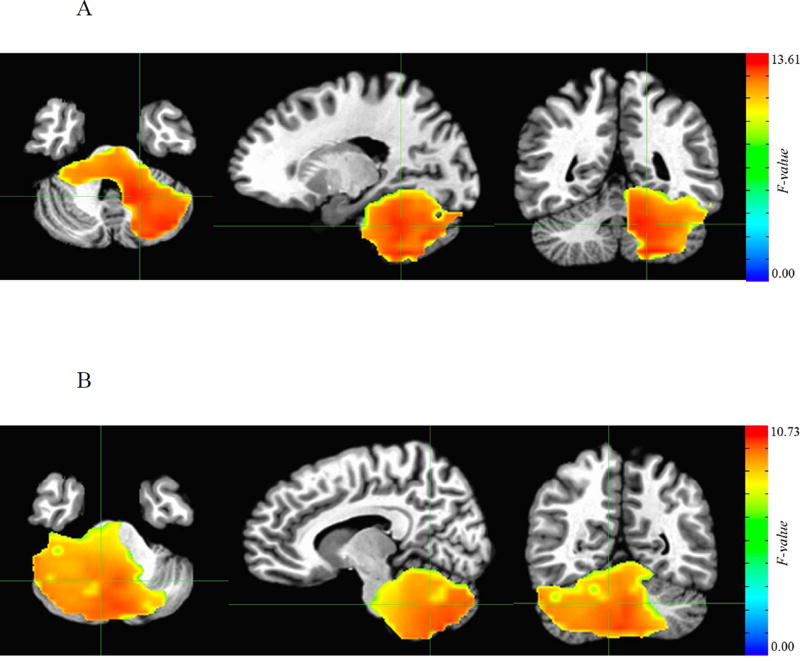
In fMRI analyses, during inhibition, right caudate anomalies reflected a childhood ADHD history and were present even among those who remitted. By contrast, differences related to adult outcome emerged in cortical (right inferior frontal and inferior parietal/precuneus) and cerebellar regions. The persistent ADHD group showed under-activation, whereas the remitted ADHD group did not differ significantly from the never-affected group. Magnetoencephalography showed that the association between adult symptom severity and prefrontal neuronal activity was confined to the time window covering the act of inhibition (300 ms-350 ms). Group differences in cerebellar and parietal neuronal activity occurred during the time window of performance monitoring processes (500 ms-600 ms).
By combining fMRI and magnetoencephalography, the location and time window of neuronal activity that underpins the adult outcome of ADHD was pinpointed. Thus, the cortico-cerebellar processes tied to the clinical course of ADHD are separated from the subcortical processes that are not.
了解与儿童注意力缺陷多动障碍(ADHD)成人期结局相关的神经过程,可为改善其临床病程的新型干预措施提供指导。有人认为,前额叶皮质活动的正常化可促使ADHD缓解,而即使在缓解期,皮质下过程的异常依然“存在”。作者利用抑制过程的多模态神经影像学,对自童年起就接受随访的成年人进行了这些假设的检验,对比了缓解型ADHD与持续性ADHD。
成年参与者(持续性ADHD,N = 35;缓解型ADHD,N = 47;从未患病,N = 99)在执行反应抑制任务期间接受了功能磁共振成像(fMRI)(N = 85)、脑磁图(N = 33)或两者(N = 63)扫描。
在fMRI分析中,抑制过程中右侧尾状核异常反映了儿童期ADHD病史,即使在缓解者中也存在。相比之下,与成人结局相关的差异出现在皮质(右侧额下回和顶下小叶/楔前叶)和小脑区域。持续性ADHD组表现为激活不足,而缓解型ADHD组与从未患病组无显著差异。脑磁图显示,成人症状严重程度与前额叶神经元活动之间的关联仅限于涵盖抑制行为的时间窗(300毫秒 - 350毫秒)。小脑和顶叶神经元活动的组间差异出现在绩效监测过程的时间窗(500毫秒 - 600毫秒)。
通过结合fMRI和脑磁图,确定了支持ADHD成人期结局的神经元活动的位置和时间窗。因此,与ADHD临床病程相关的皮质 - 小脑过程与不相关的皮质下过程是分开的。