Ghoshal Uday C
Department of Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India.
J Neurogastroenterol Motil. 2017 Jul 30;23(3):334-340. doi: 10.5056/jnm17020.
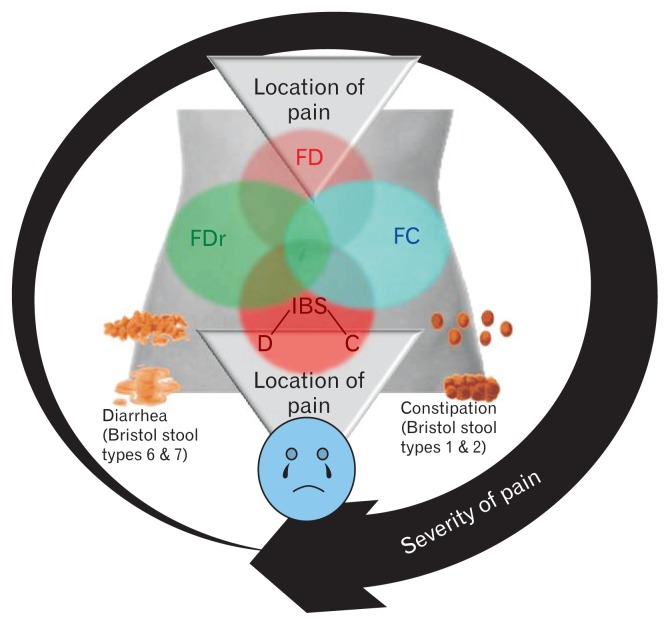
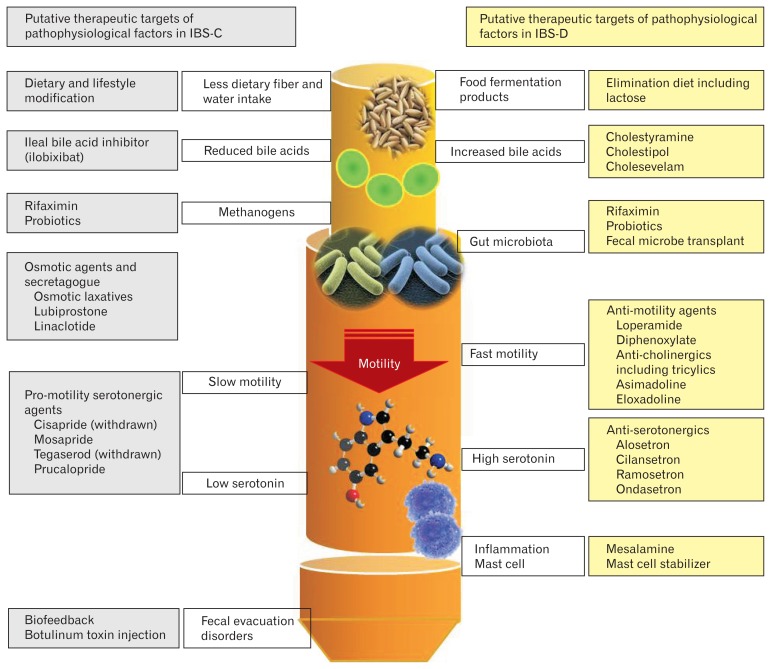
A decade after Rome III, in 2016, Rome IV criteria were published. There are major differences between Rome IV and the earlier iteration, some of which are in line with Asian viewpoints. The clinical applicability of the Rome IV criteria of irritable bowel syndrome (IBS) in Asian perspective is reviewed here. Instead of considering functional gastrointestinal disorders (FGIDs) to be largely psychogenic, Rome IV suggested the importance of the gut over brain ("disorders of gut-brain interaction" not "brain-gut interaction"). The word "functional" is underplayed. Multi-dimensional clinical profile attempts to recognize micro-organic nature, like slow colon transit and fecal evacuation disorders in constipation and dietary intolerance including that of lactose and fructose, bile acid malabsorption, non-celiac wheat sensitivity, small intestinal bacterial overgrowth, and gastrointestinal infection in diarrhea. Overlap between different FGIDs has been recognized as Rome IV suggests these to be a spectrum rather than discrete disorders. Bloating, common in Asia, received attention, though less. Sub-typing of IBS may be more clinician-friendly now as the patient-reported stool form may be used than a diary. However, a few issues, peculiar to Asia, need consideration; Rome IV, like Rome III, suggests that Bristol type I-II stool to denote constipation though Asian experts include type III as well. Work-up for physiological factors should be given greater importance. Language issue is important. Bloating, common in IBS, should be listed in the criteria. Threshold values for symptoms in Rome IV criteria are based on Western data. Post-infectious malabsorption (tropical sprue) should be excluded to diagnose post-infectious IBS, particularly in Asia.
在罗马Ⅲ标准发布十年后的2016年,罗马Ⅳ标准问世。罗马Ⅳ标准与早期版本存在重大差异,其中一些与亚洲观点相符。本文将从亚洲视角审视罗马Ⅳ标准中肠易激综合征(IBS)的临床适用性。罗马Ⅳ标准不再认为功能性胃肠疾病(FGIDs)主要是心因性的,而是提出了肠道优于大脑的重要性(“肠-脑相互作用障碍”而非“脑-肠相互作用”)。“功能性”一词的重要性被淡化。多维临床概况试图识别微观有机性质,如便秘时的结肠传输缓慢和粪便排出障碍,以及腹泻时的饮食不耐受,包括乳糖和果糖不耐受、胆汁酸吸收不良、非乳糜泻性小麦敏感、小肠细菌过度生长和胃肠道感染。罗马Ⅳ标准认识到不同FGIDs之间存在重叠,认为它们是一个连续谱而非离散的疾病。在亚洲常见的腹胀虽受到关注,但较少。现在IBS的亚型分类可能对临床医生更友好,因为可以使用患者报告的粪便形态而非日记。然而,一些亚洲特有的问题需要考虑;与罗马Ⅲ标准一样,罗马Ⅳ标准认为布里斯托Ⅰ-Ⅱ型粪便表示便秘,而亚洲专家也将Ⅲ型包括在内。应更重视对生理因素的检查。语言问题很重要。IBS中常见的腹胀应列入标准。罗马Ⅳ标准中症状的阈值基于西方数据。诊断感染后IBS时应排除感染后吸收不良(热带口炎性腹泻),在亚洲尤其如此。