Division of Medical Oncology, Department of Medical Oncology, GROW-School for Oncology and Developmental Biology, Maastricht University Medical Centre, P.O. Box 5800, 6202 AZ, Maastricht, The Netherlands.
Comprehensive Cancer Centre the Netherlands, Nijmegen, The Netherlands.
Breast Cancer Res Treat. 2017 Oct;165(3):593-600. doi: 10.1007/s10549-017-4364-8. Epub 2017 Jul 3.
The INTENS study was designed to determine whether delivering neoadjuvant chemotherapy at a higher dose in a shorter period of time improves outcome of breast cancer patients.
Women with newly diagnosed breast cancer were randomly assigned to neoadjuvant chemotherapy consisting of four cycles of doxorubicin and cyclophosphamide followed by four cycles of docetaxel (AC 60/600-T 100 mg/m) or six cycles of TAC as triplet chemotherapy (75/50/500 mg/m) every 3 weeks. The primary outcome was the pathologic complete response (pCR), with disease-free and overall survival as secondary endpoints.
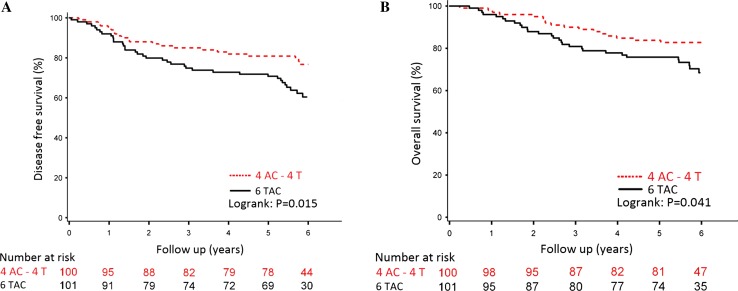
In total, 201 patients were included. The pCR rates were 28% for patients treated with AC-T and 19% for patients treated with TAC, with an odds ratio of 1.60 (95% CI 0.90-3.21). With a median follow-up of 6 years (range 0.04-8.41 years), the five-year disease-free survival was 81% for patients treated with sequentially AC-T and 71% for patients treated with concurrent triplet TAC chemotherapy with a stratified hazard ratio (HR) of 0.50 (95% CI 0.29-0.86). Five-year overall survival was 84% versus 76%, respectively, with a stratified HR of 0.55 (95% CI 0.29-1.03).
No differences were observed between the two treatment arms with respect to pCR rate, but the sequentially delivered chemotherapy outperformed the triplet combination chemotherapy in terms of survival, despite a lower cumulative dose per agent. GOV nr NCT00314977.
INTENS 研究旨在确定在更短的时间内以更高剂量给予新辅助化疗是否能改善乳腺癌患者的预后。
新诊断为乳腺癌的女性被随机分配接受新辅助化疗,方案为阿霉素和环磷酰胺 4 个周期,随后多西他赛 4 个周期(AC60/600-T100mg/m)或三药联合 TAC(75/50/500mg/m)6 个周期,每 3 周 1 次。主要终点为病理完全缓解(pCR),无病生存和总生存为次要终点。
共纳入 201 例患者。AC-T 组和 TAC 组的 pCR 率分别为 28%和 19%,优势比为 1.60(95%CI 0.90-3.21)。中位随访 6 年(范围 0.04-8.41 年),AC-T 序贯治疗组 5 年无病生存率为 81%,同期三药联合 TAC 化疗组为 71%,分层风险比(HR)为 0.50(95%CI 0.29-0.86)。5 年总生存率分别为 84%和 76%,分层 HR 为 0.55(95%CI 0.29-1.03)。
两组间 pCR 率无差异,但序贯化疗在生存方面优于三药联合化疗,尽管每个药物的累积剂量较低。GOV nr NCT00314977。