aDivision of Biokinesiology and Physical Therapy, University of Southern California, Los Angeles, CA, USAbDepartment of Anesthesiology, Chronic Pain and Fatigue Research Center, University of Michigan, Ann Arbor, MI, USAcOppenheimer Center for Neurobiology of Stress, Pain and Interoception Network (PAIN), David Geffen School of Medicine at UCLA, Los Angeles, CA, USAdDepartment of Physiology, Northwestern University, Feinberg School of Medicine, Chicago, IL, USAeDepartment of Anesthesiology, Perioperative and Pain Medicine, Division of Pain Medicine, Stanford University Medical Center, Stanford, CA, USAfDepartments of Radiology and Anesthesiology, University of Alabama, Birmingham Medical Center, Birmingham, AL, USAgDepartment of Urology, Northwestern University, Feinberg School of Medicine, Chicago, IL, USAhDepartment of Urology, University of Southern California, Los Angeles, CA, USAiDepartment of Urology, University of Iowa, Iowa City, IA, USAjCollege of Medicine, Washington State University, Seattle, WA, USAkDepartment of Urology, Washington University, Saint Louis, MO, USAlNational Institute of Diabetes and Digestive and Kidney Diseases, NIH, Bethesda, MD, USAmDepartment of Biostatistics and Epidemiology, University of Pennsylvania, Philadelphia, PA, USAnDepartment of Urology, University of Michigan, Ann Arbor, MI, USA.
Pain. 2017 Oct;158(10):1979-1991. doi: 10.1097/j.pain.0000000000001001.
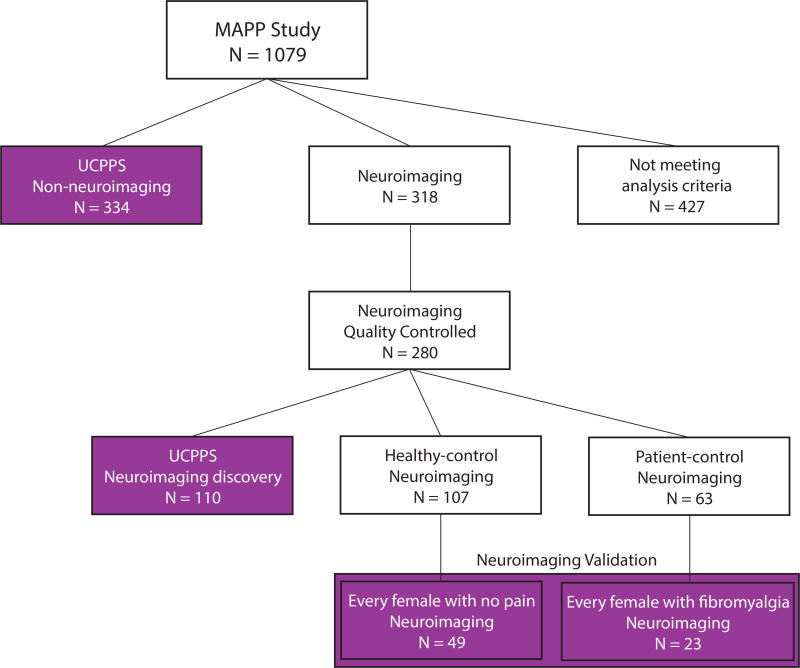
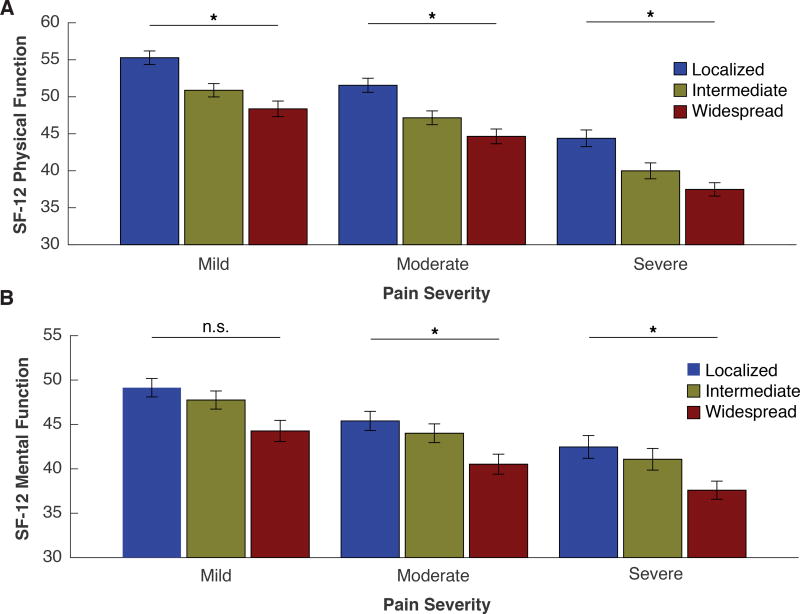
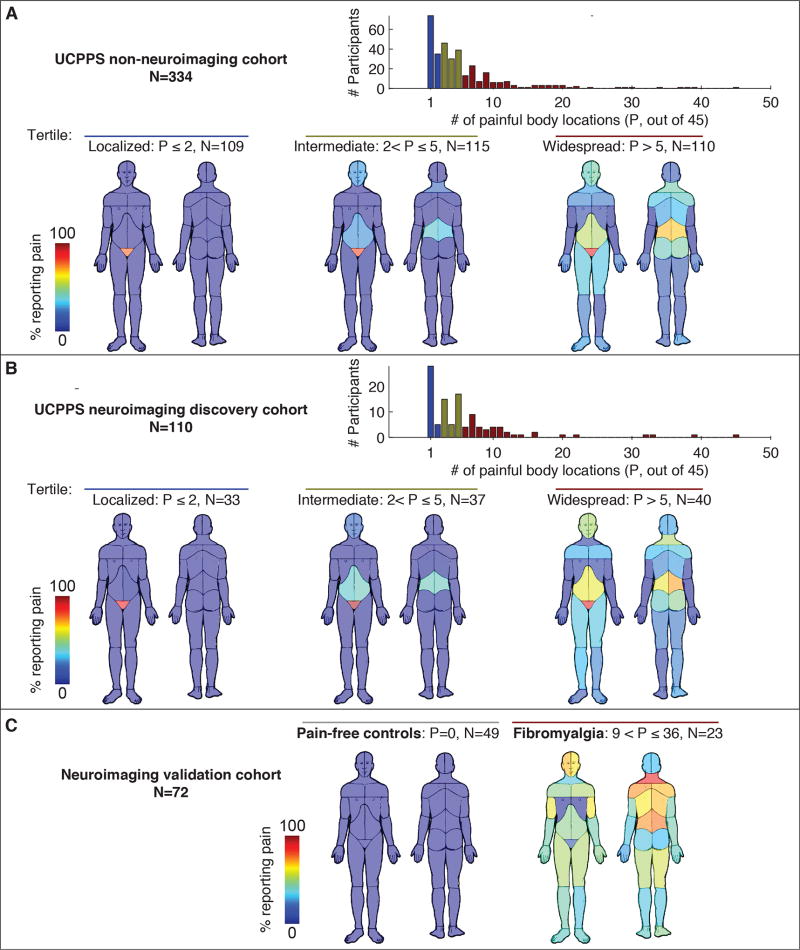
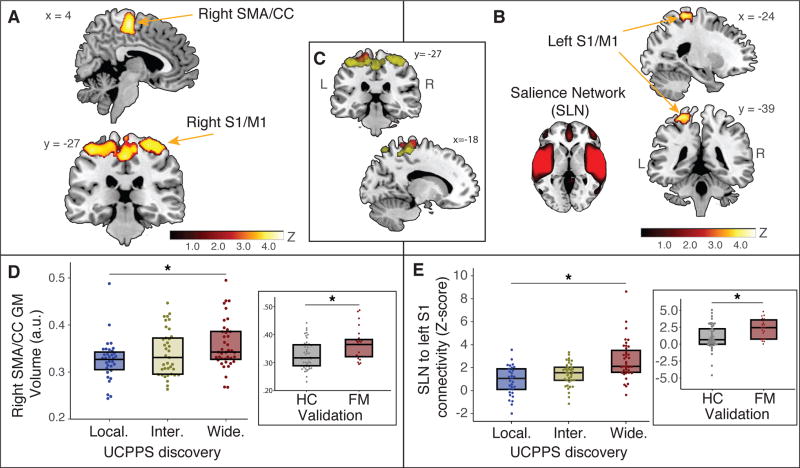
Chronic pain is often measured with a severity score that overlooks its spatial distribution across the body. This widespread pain is believed to be a marker of centralization, a central nervous system process that decouples pain perception from nociceptive input. Here, we investigated whether centralization is manifested at the level of the brain using data from 1079 participants in the Multidisciplinary Approach to the Study of Chronic Pelvic Pain Research Network (MAPP) study. Participants with a clinical diagnosis of urological chronic pelvic pain syndrome (UCPPS) were compared to pain-free controls and patients with fibromyalgia, the prototypical centralized pain disorder. Participants completed questionnaires capturing pain severity, function, and a body map of pain. A subset (UCPPS N = 110; fibromyalgia N = 23; healthy control N = 49) underwent functional and structural magnetic resonance imaging. Patients with UCPPS reported pain ranging from localized (pelvic) to widespread (throughout the body). Patients with widespread UCPPS displayed increased brain gray matter volume and functional connectivity involving sensorimotor and insular cortices (P < 0.05 corrected). These changes translated across disease diagnoses as identical outcomes were present in patients with fibromyalgia but not pain-free controls. Widespread pain was also associated with reduced physical and mental function independent of pain severity. Brain pathology in patients with centralized pain is related to pain distribution throughout the body. These patients may benefit from interventions targeting the central nervous system.
慢性疼痛通常用严重程度评分来衡量,但这种评分忽略了其在全身的空间分布。这种广泛的疼痛被认为是集中化的标志,这是一种中枢神经系统过程,它将疼痛感知与伤害性输入解耦。在这里,我们使用来自多学科慢性盆腔疼痛研究网络(MAPP)研究的 1079 名参与者的数据,研究了集中化是否在大脑水平上表现出来。与疼痛组相比,患有尿路上皮性慢性盆腔疼痛综合征(UCPPS)的参与者与疼痛对照组和纤维肌痛患者进行了比较,纤维肌痛是典型的集中性疼痛障碍。参与者完成了问卷,包括疼痛严重程度、功能和疼痛身体图。一小部分(UCPPS N = 110;纤维肌痛 N = 23;健康对照组 N = 49)接受了功能和结构磁共振成像。UCPPS 患者报告的疼痛范围从局部(盆腔)到广泛(全身)。广泛性 UCPPS 患者显示大脑灰质体积增加,涉及感觉运动和脑岛皮层的功能连接增强(校正后 P < 0.05)。这些变化跨越疾病诊断存在,因为纤维肌痛患者和非疼痛对照组患者存在相同的结果。广泛的疼痛也与身体和精神功能下降有关,而与疼痛严重程度无关。集中性疼痛患者的大脑病理学与全身疼痛分布有关。这些患者可能受益于针对中枢神经系统的干预措施。