aDepartment of Pharmacotherapy, University of Utah College of Pharmacy bInformatics, Decision-Enhancement, and Surveillance (IDEAS) Center, Salt Lake City VA Health Care System cDepartment of Population Health Sciences, University of Utah, Salt Lake City, Utah dBristol-Myers Squibb, Lawrenceville, New Jersey eDivision of Epidemiology, Department of Internal Medicine, University of Utah, Salt Lake City, Utah fDepartment of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, USA.
AIDS. 2017 Sep 24;31(15):2095-2106. doi: 10.1097/QAD.0000000000001594.
Patients with HIV infection have an increased risk of cardiovascular disease compared with uninfected individuals. Antiretroviral therapy with atazanavir (ATV) delays progression of atherosclerosis markers; whether this reduces cardiovascular disease event risk compared with other antiretroviral regimens is currently unknown.
Population-based, noninterventional, historical cohort study conducted from 1 July 2003 through 31 December 2015.
Veterans Health Administration hospitals and clinics throughout the United States.
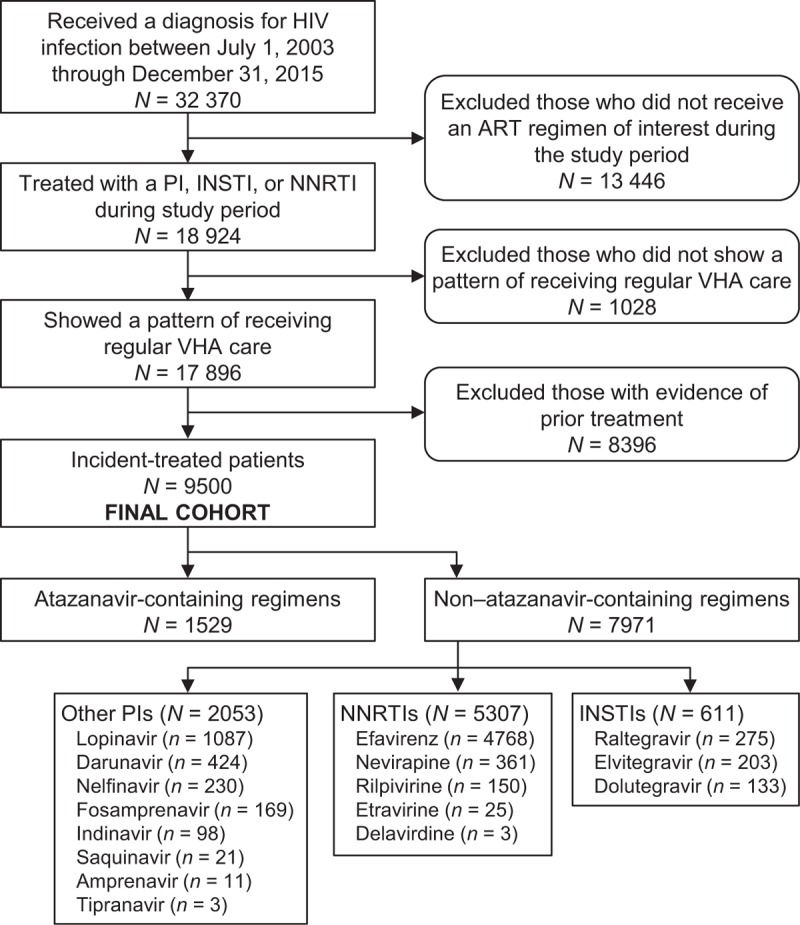
Treatment-naive patients with HIV infection (N = 9500).
Initiating antiretroviral regimens containing ATV, other protease inhibitors, nonnucleoside reverse transcriptase inhibitors (NNRTIs), or integrase strand transfer inhibitors (INSTIs).
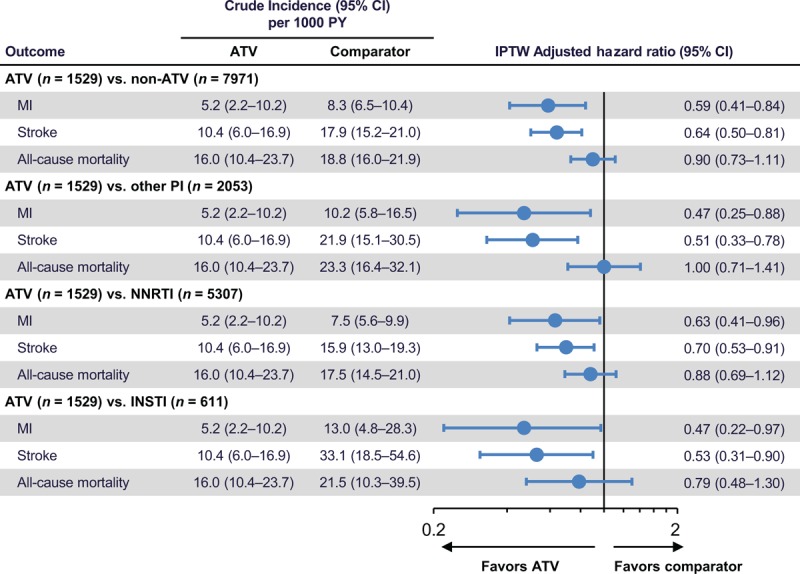
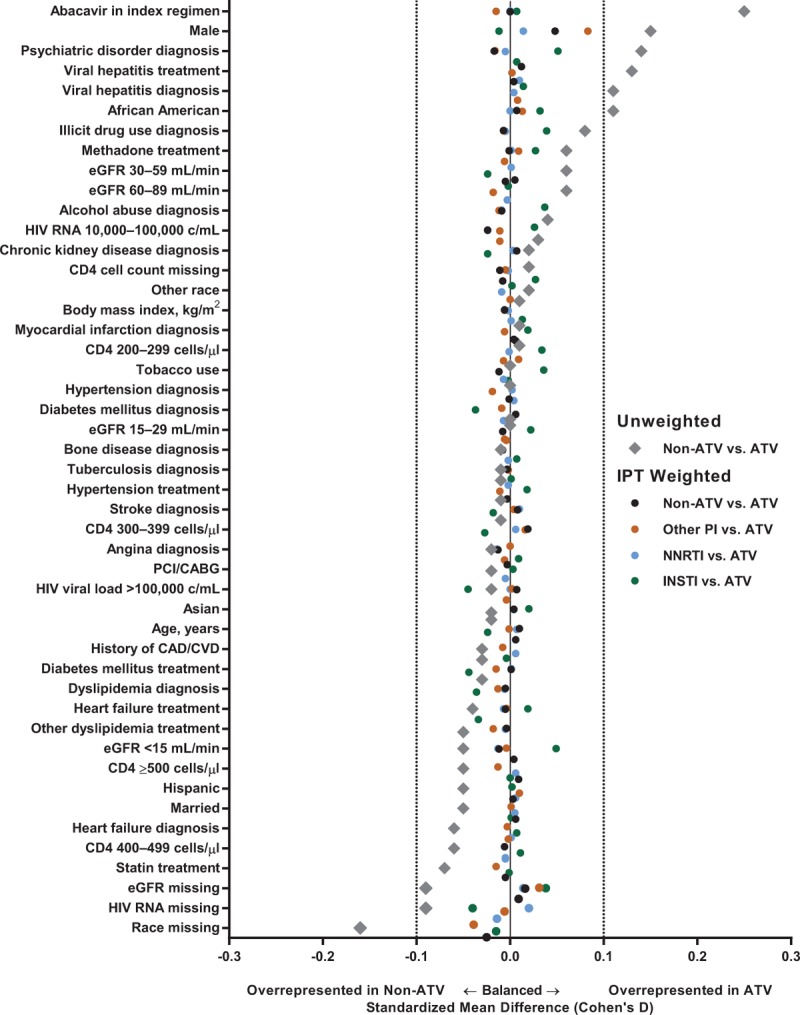
MAIN OUTCOME/EFFECT SIZE MEASURES: Incidence rates of myocardial infarction (MI), stroke, and all-cause mortality within each regimen. ATV versus other protease inhibitor, NNRTI, or INSTI covariate-adjusted hazard ratios by using Cox proportional hazards models and inverse probability of treatment weighting.
Incidence rates for MI, stroke, and all-cause mortality with ATV-containing regimens (5.2, 10.4, and 16.0 per 1000 patient-years, respectively) were lower than with regimens containing other protease inhibitors (10.2, 21.9, and 23.3 per 1000 patient-years), NNRTIs (7.5, 15.9, and 17.5 per 1000 patient-years), or INSTIs (13.0, 33.1, and 21.5 per 1000 patient-years). After inverse probability of treatment weighting, adjusted hazard ratios (95% confidence intervals) for MI, stroke, and all-cause mortality with ATV-containing regimens versus all non-ATV-containing regimens were 0.59 (0.41-0.84), 0.64 (0.50-0.81), and 0.90 (0.73-1.11), respectively.
Among treatment-naive HIV-infected patients in the Veterans Health Administration initiating ATV-containing regimens, risk of both MI and stroke were significantly lower than in those initiating regimens containing other protease inhibitors, NNRTIs, or INSTIs.
与未感染个体相比,HIV 感染者发生心血管疾病的风险增加。阿扎那韦(ATV)的抗逆转录病毒治疗可延缓动脉粥样硬化标志物的进展;与其他抗逆转录病毒方案相比,这是否降低了心血管疾病事件的风险目前尚不清楚。
从 2003 年 7 月 1 日至 2015 年 12 月 31 日进行的基于人群的非干预性历史队列研究。
美国退伍军人健康管理局的医院和诊所。
初治 HIV 感染患者(N=9500)。
开始使用含有 ATV、其他蛋白酶抑制剂、非核苷类逆转录酶抑制剂(NNRTIs)或整合酶链转移抑制剂(INSTIs)的抗逆转录病毒方案。
主要结局/效应大小测量指标:每种方案中心肌梗死(MI)、中风和全因死亡率的发生率。使用 Cox 比例风险模型和逆概率治疗加权法,对 ATV 与其他蛋白酶抑制剂、NNRTI 或 INSTI 的协变量调整后的危险比进行评估。
含 ATV 方案的 MI、中风和全因死亡率发生率(分别为 5.2、10.4 和 16.0/1000 患者年)低于含其他蛋白酶抑制剂(10.2、21.9 和 23.3/1000 患者年)、NNRTIs(7.5、15.9 和 17.5/1000 患者年)或 INSTIs(13.0、33.1 和 21.5/1000 患者年)的方案。经过治疗逆概率加权后,与所有非 ATV 方案相比,含 ATV 方案治疗的 MI、中风和全因死亡率的调整后的危险比(95%置信区间)分别为 0.59(0.41-0.84)、0.64(0.50-0.81)和 0.90(0.73-1.11)。
在开始使用含 ATV 方案的初治 HIV 感染患者中,MI 和中风的风险均明显低于开始使用其他蛋白酶抑制剂、NNRTIs 或 INSTIs 方案的患者。