Main Keith L, Soman Salil, Pestilli Franco, Furst Ansgar, Noda Art, Hernandez Beatriz, Kong Jennifer, Cheng Jauhtai, Fairchild Jennifer K, Taylor Joy, Yesavage Jerome, Wesson Ashford J, Kraemer Helena, Adamson Maheen M
War Related Illness and Injury Study Center, Veterans Affairs, Palo Alto Health Care System (VAPAHCS), Palo Alto, CA, United States.
Defense and Veterans Brain Injury Center (DVBIC), Silver Spring, MD, United States.
Neuroimage Clin. 2017 Jun 24;16:1-16. doi: 10.1016/j.nicl.2017.06.031. eCollection 2017.
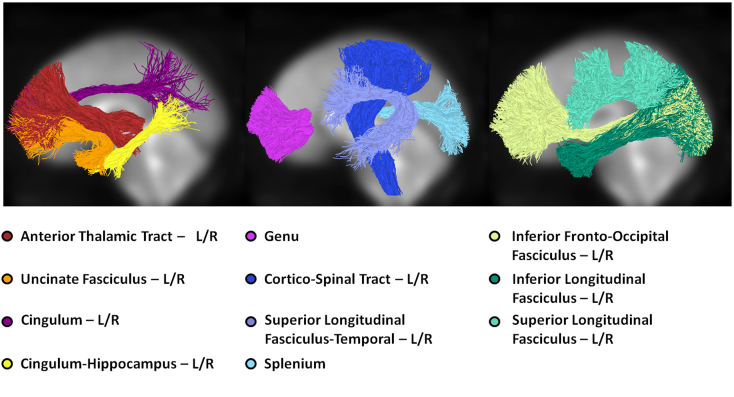
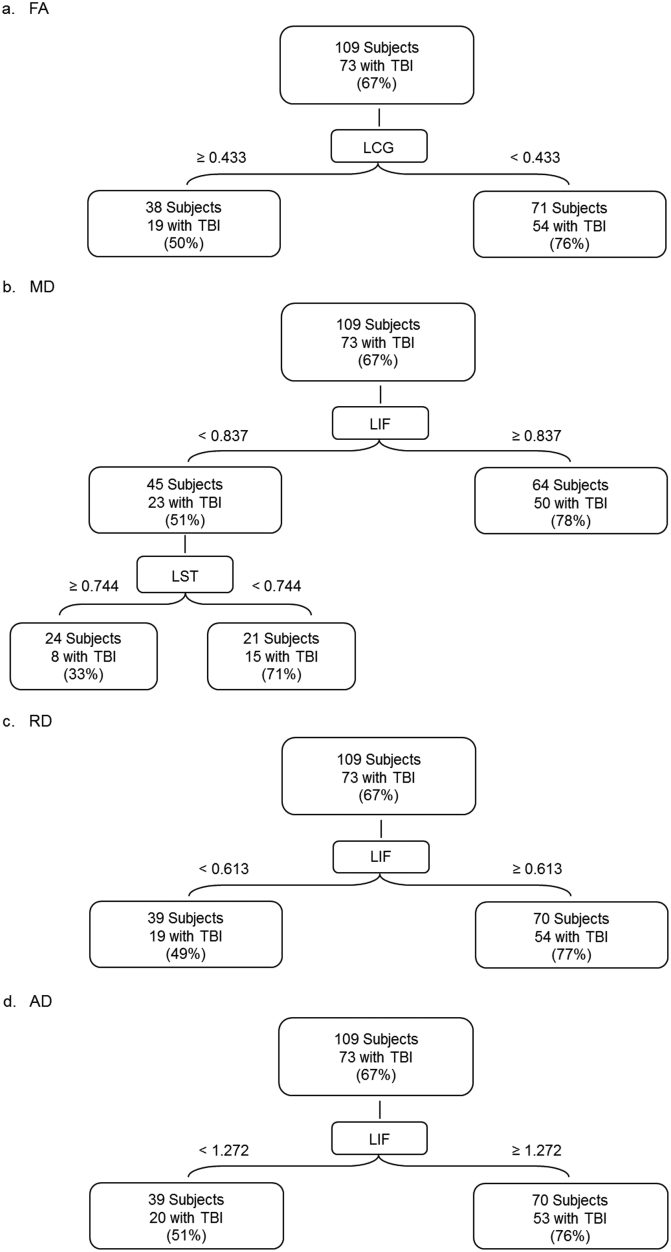
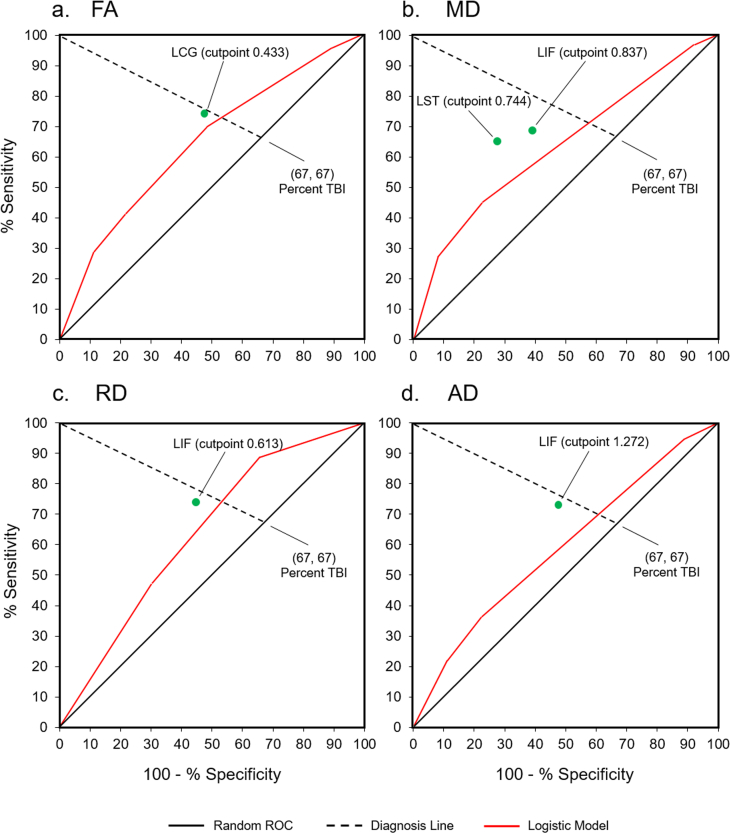
Standard MRI methods are often inadequate for identifying mild traumatic brain injury (TBI). Advances in diffusion tensor imaging now provide potential biomarkers of TBI among white matter fascicles (tracts). However, it is still unclear which tracts are most pertinent to TBI diagnosis. This study ranked fiber tracts on their ability to discriminate patients with and without TBI. We acquired diffusion tensor imaging data from military veterans admitted to a polytrauma clinic (Overall = 109; Age: = 47.2, = 11.3; Male: 88%; TBI: 67%). TBI diagnosis was based on self-report and neurological examination. Fiber tractography analysis produced 20 fiber tracts per patient. Each tract yielded four clinically relevant measures (fractional anisotropy, mean diffusivity, radial diffusivity, and axial diffusivity). We applied receiver operating characteristic (ROC) analyses to identify the most diagnostic tract for each measure. The analyses produced an optimal cutpoint for each tract. We then used kappa coefficients to rate the agreement of each cutpoint with the neurologist's diagnosis. The tract with the highest kappa was most diagnostic. As a check on the ROC results, we performed a stepwise logistic regression on each measure using all 20 tracts as predictors. We also bootstrapped the ROC analyses to compute the 95% confidence intervals for sensitivity, specificity, and the highest kappa coefficients. The ROC analyses identified two fiber tracts as most diagnostic of TBI: the left cingulum (LCG) and the left inferior fronto-occipital fasciculus (LIF). Like ROC, logistic regression identified LCG as most predictive for the FA measure but identified the right anterior thalamic tract (RAT) for the MD, RD, and AD measures. These findings are potentially relevant to the development of TBI biomarkers. Our methods also demonstrate how ROC analysis may be used to identify clinically relevant variables in the TBI population.
标准的磁共振成像(MRI)方法往往不足以识别轻度创伤性脑损伤(TBI)。扩散张量成像技术的进展现在为白质束(神经纤维束)中的TBI提供了潜在的生物标志物。然而,目前仍不清楚哪些神经纤维束与TBI诊断最为相关。本研究根据纤维束区分TBI患者和非TBI患者的能力对其进行了排名。我们从一家多创伤诊所收治的退伍军人中获取了扩散张量成像数据(总计109人;年龄:47.2岁,标准差11.3岁;男性:88%;TBI:67%)。TBI诊断基于自我报告和神经学检查。纤维束成像分析为每位患者生成了20条纤维束。每条纤维束产生四个临床相关指标(各向异性分数、平均扩散率、径向扩散率和轴向扩散率)。我们应用了受试者操作特征(ROC)分析来确定每个指标最具诊断性的纤维束。分析为每条纤维束产生了一个最佳切点。然后,我们使用kappa系数来评估每个切点与神经科医生诊断的一致性。kappa值最高的纤维束诊断价值最大。作为对ROC结果的检验,我们对每个指标进行了逐步逻辑回归,将所有20条纤维束作为预测变量。我们还对ROC分析进行了自抽样,以计算敏感性、特异性和最高kappa系数的95%置信区间。ROC分析确定了两条纤维束对TBI最具诊断性:左侧扣带束(LCG)和左侧额枕下束(LIF)。与ROC分析一样,逻辑回归确定LCG对FA指标最具预测性,但对MD、RD和AD指标确定右侧丘脑前束(RAT)最具预测性。这些发现可能与TBI生物标志物的开发相关。我们的方法还展示了如何使用ROC分析来识别TBI人群中的临床相关变量。