Pollack Craig Evan, Armstrong Katrina A, Mitra Nandita, Chen Xinwei, Ward Katelyn R, Radhakrishnan Archana, Wong Michelle S, Bekelman Justin E, Branas Charles C, Rhodes Karin V, Grande David T
Division of General Internal Medicine, Johns Hopkins School of Medicine, Baltimore, Maryland.
Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Cancer. 2017 Nov 15;123(22):4449-4457. doi: 10.1002/cncr.30894. Epub 2017 Jul 20.
Racial disparities in prostate cancer treatment and outcomes are widespread and poorly understood. In the current study, the authors sought to determine whether access to care, measured across multiple dimensions, contributed to racial differences in prostate cancer.
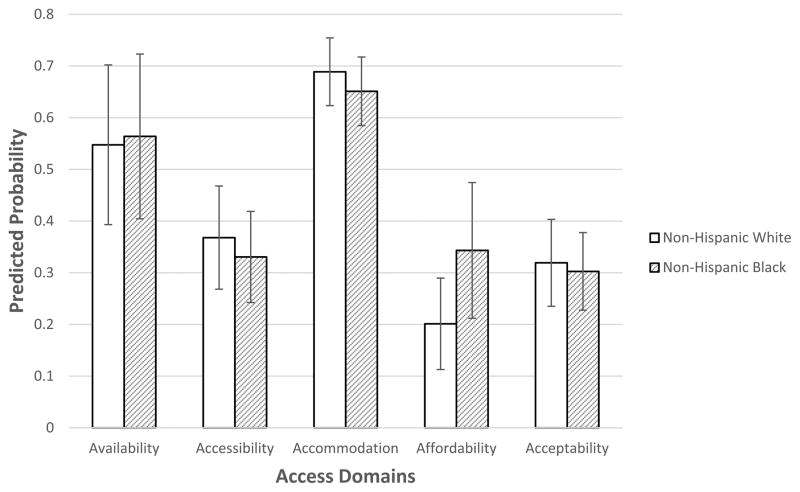
The Philadelphia Area Prostate Cancer Access Study (P Access) included 2374 men diagnosed with localized prostate cancer between 2012 and 2014. Men were surveyed to assess their experiences accessing care (response rate of 51.1%). The authors determined appointment availability at 151 urology practices using simulated patient telephone calls and calculated travel distances using geospatial techniques. Multivariable logistic regression models were used to determine the association between 5 different domains of access (availability, accessibility, accommodation, affordability, and acceptability) and receipt of treatment, perceived quality of care, and physician-patient communication.
There were 1907 non-Hispanic white and 394 black men in the study cohort. Overall, approximately 85% of the men received definitive treatment with no differences noted by race. Black men were less likely to report a high quality of care (69% vs 81%; P<.001) and good physician-patient communication (60% vs 71%; P<.001) compared with white men. In adjusted models, none of the 5 domains of access were found to be associated with definitive treatment overall or with radical prostatectomy. All access domains were associated with perceived quality of care and communication, although these domains did not mediate racial disparities.
To the authors' knowledge, the current study presents the first comprehensive assessment of prostate cancer care access, treatment, and patient experience, demonstrating that although access was related to overall perceived quality of care and better physician-patient communication, it did not appear to explain observed racial differences. Cancer 2017;123:4449-57. © 2017 American Cancer Society.
前列腺癌治疗及预后方面的种族差异普遍存在且鲜为人知。在本研究中,作者试图确定从多个维度衡量的医疗服务可及性是否导致了前列腺癌的种族差异。
费城地区前列腺癌可及性研究(P Access)纳入了2012年至2014年间被诊断为局限性前列腺癌的2374名男性。对这些男性进行了调查,以评估他们获得医疗服务的经历(应答率为51.1%)。作者通过模拟患者电话访问确定了151家泌尿外科诊所的预约可得性,并使用地理空间技术计算了出行距离。多变量逻辑回归模型用于确定5个不同的可及性领域(可得性、可达性、适应性、可负担性和可接受性)与治疗接受情况、感知的医疗质量以及医患沟通之间的关联。
研究队列中有1907名非西班牙裔白人男性和394名黑人男性。总体而言,约85%的男性接受了确定性治疗,未观察到种族差异。与白人男性相比,黑人男性报告高质量医疗服务的可能性较小(69%对81%;P<0.001),且医患沟通良好的可能性也较小(60%对71%;P<0.001)。在调整后的模型中,未发现5个可及性领域中的任何一个与总体确定性治疗或根治性前列腺切除术相关。所有可及性领域均与感知的医疗质量和沟通相关,尽管这些领域并未介导种族差异。
据作者所知,本研究首次对前列腺癌医疗服务可及性、治疗及患者体验进行了全面评估,表明尽管可及性与总体感知的医疗质量及更好的医患沟通相关,但似乎无法解释所观察到的种族差异。《癌症》2017年;123:4449 - 57。©2017美国癌症协会。