Sales Arthur H A, Barz Melanie, Bette Stefanie, Wiestler Benedikt, Ryang Yu-Mi, Meyer Bernhard, Bretschneider Martin, Ringel Florian, Gempt Jens
Department of Neurosurgery, Klinikum rechts der Isar, Technical University of Munich, Ismaninger Str. 22, 81675, Munich, Germany.
Department of Neuroradiology, Klinikum rechts der Isar, Technical University of Munich, Ismaninger Str. 22, 81675, Munich, Germany.
BMC Med. 2017 Jul 25;15(1):137. doi: 10.1186/s12916-017-0898-1.
Postoperative ischemia is a frequent phenomenon in patients with brain tumors and is associated with postoperative neurological deficits and impaired overall survival. Particularly in the field of cardiac and vascular surgery, the application of a brief ischemic stimulus not only in the target organ but also in remote tissues can prevent subsequent ischemic damage. We hypothesized that remote ischemic preconditioning (rIPC) in patients with brain tumors undergoing elective surgical resection reduces the incidence of postoperative ischemic tissue damage and its consequences.
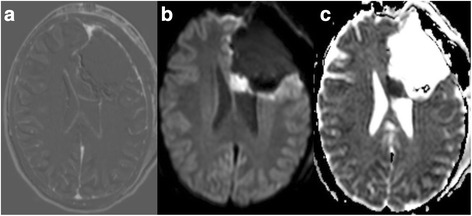
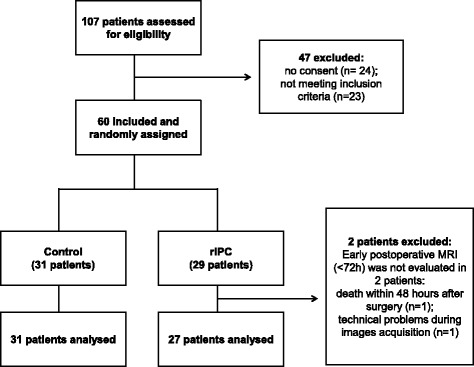
Sixty patients were randomly assigned to two groups, with 1:1 allocation, stratified by tumor type (glioma or metastasis) and previous treatment with radiotherapy. rIPC was induced by inflating a blood pressure cuff placed on the upper arm three times for 5 min at 200 mmHg in the treatment group after induction of anesthesia. Between the cycles, the blood pressure cuff was released to allow reperfusion. In the control group no preconditioning was performed. Early postoperative magnetic resonance images (within 72 h after surgery) were evaluated by a neuroradiologist blinded to randomization for the presence of ischemia and its volume.
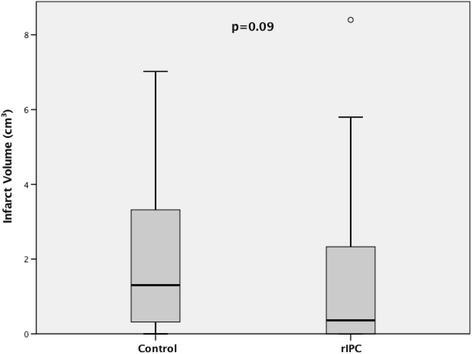
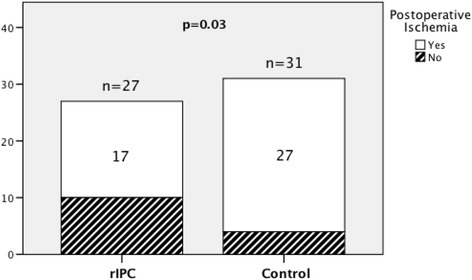
Fifty-eight of the 60 patients were assessed for occurrence of postoperative ischemia. Of these 58 patients, 44 had new postoperative ischemic lesions. The incidence of new postoperative ischemic lesions was significantly higher in the control group (27/31) than in the rIPC group (17/27) (p = 0.03). The median infarct volume was 0.36 cm (interquartile range (IR): 0.0-2.35) in the rIPC group compared with 1.30 cm (IR: 0.29-3.66) in the control group (p = 0.09).
Application of rIPC was associated with reduced incidence of postoperative ischemic tissue damage in patients undergoing elective brain tumor surgery. This is the first study indicating a benefit of rIPC in brain tumor surgery.
German Clinical Trials Register, DRKS00010409 . Retrospectively registered on 13 October 2016.
术后缺血是脑肿瘤患者常见的现象,与术后神经功能缺损及总体生存率受损相关。特别是在心脏和血管外科领域,短暂缺血刺激不仅应用于靶器官,也应用于远处组织,可预防随后的缺血损伤。我们假设,对接受择期手术切除的脑肿瘤患者进行远隔缺血预处理(rIPC)可降低术后缺血性组织损伤的发生率及其后果。
60例患者按1:1比例随机分为两组,按肿瘤类型(胶质瘤或转移瘤)及既往放疗治疗情况进行分层。麻醉诱导后,治疗组在上臂放置血压袖带,以200 mmHg充气3次,每次5分钟,诱导rIPC。两次充气之间,松开血压袖带以实现再灌注。对照组不进行预处理。术后早期磁共振成像(术后72小时内)由一位对随机分组不知情的神经放射科医生评估是否存在缺血及其体积。
60例患者中有58例接受了术后缺血情况评估。在这58例患者中,44例出现了新的术后缺血性病变。对照组新的术后缺血性病变发生率(27/31)显著高于rIPC组(17/27)(p = 0.03)。rIPC组梗死体积中位数为0.36 cm(四分位间距(IR):0.0 - 2.35),而对照组为1.30 cm(IR:0.29 - 3.66)(p = 0.09)。
rIPC的应用与接受择期脑肿瘤手术患者术后缺血性组织损伤发生率降低相关。这是第一项表明rIPC在脑肿瘤手术中有益的研究。
德国临床试验注册中心,DRKS00010409。于2016年10月13日进行回顾性注册。