Térémetz Maxime, Carment Loïc, Brénugat-Herne Lindsay, Croca Marta, Bleton Jean-Pierre, Krebs Marie-Odile, Maier Marc A, Amado Isabelle, Lindberg Påvel G
FR3636, CNRS, Université Paris Descartes, Sorbonne Paris Cité, Paris, France.
SHU, Resource Center for Cognitive Remediation and Psychosocial Rehabilitation, Université Paris Descartes, Hôpital Sainte-Anne, Paris, France.
Front Psychiatry. 2017 Jul 10;8:120. doi: 10.3389/fpsyt.2017.00120. eCollection 2017.
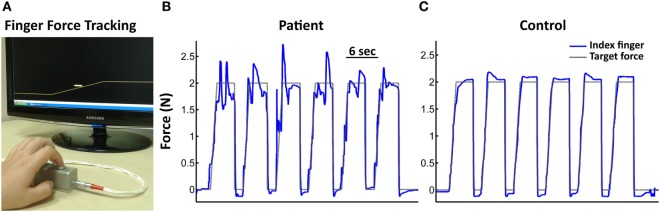
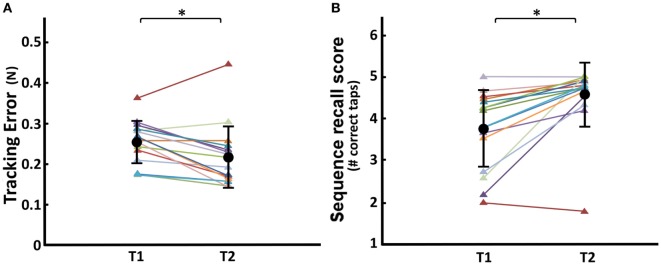
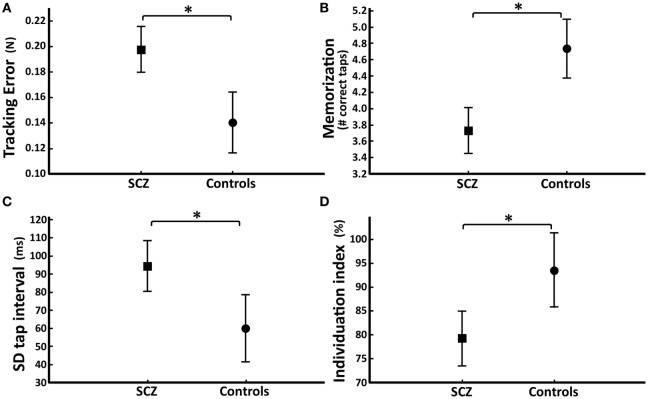
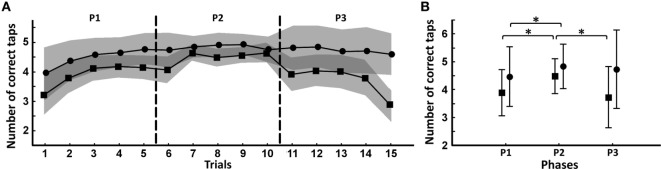
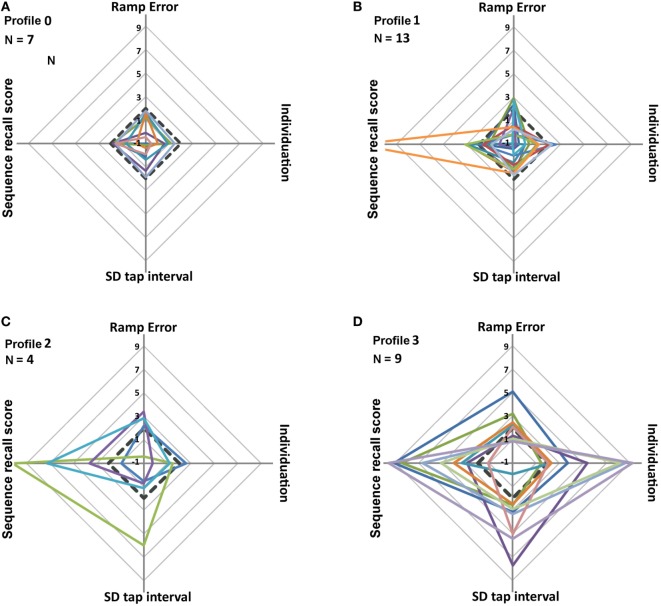
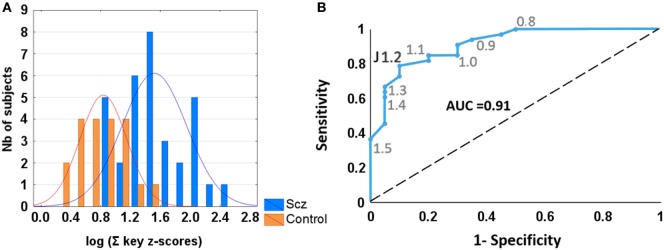
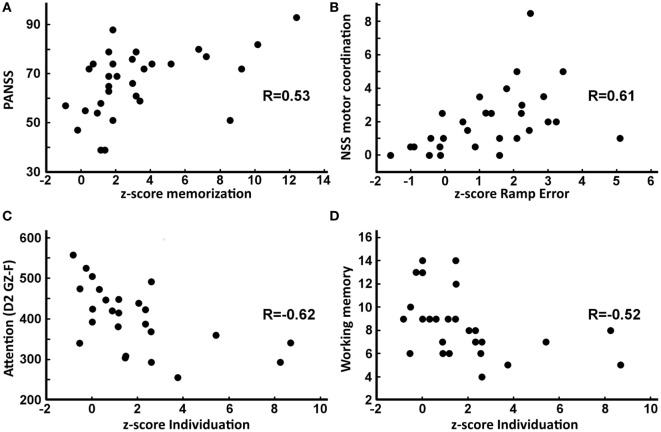
Impaired manual dexterity is commonly observed in schizophrenia. However, a quantitative description of key sensorimotor components contributing to impaired dexterity is lacking. Whether the key components of dexterity are differentially affected and how they relate to clinical characteristics also remains unclear. We quantified the degree of dexterity in 35 stabilized patients with schizophrenia and in 20 age-matched control subjects using four visuomotor tasks: (i) force tracking to quantify visuomotor precision, (ii) sequential finger tapping to measure motor sequence recall, (iii) single-finger tapping to assess temporal regularity, and (iv) multi-finger tapping to measure independence of finger movements. Diverse clinical and neuropsychological tests were also applied. A patient subgroup ( = 15) participated in a 14-week cognitive remediation protocol and was assessed before and after remediation. Compared to control subjects, patients with schizophrenia showed greater error in force tracking, poorer recall of tapping sequences, decreased tapping regularity, and reduced degree of finger individuation. A composite performance measure discriminated patients from controls with sensitivity = 0.79 and specificity = 0.9. Aside from force-tracking error, no other dexterity components correlated with antipsychotic medication. In patients, some dexterity components correlated with neurological soft signs, Positive and Negative Syndrome Scale (PANSS), or neuropsychological scores. This suggests differential cognitive contributions to these components. Cognitive remediation lead to significant improvement in PANSS, tracking error, and sequence recall (without change in medication). These findings show that multiple aspects of sensorimotor control contribute to impaired manual dexterity in schizophrenia. Only visuomotor precision was related to antipsychotic medication. Good diagnostic accuracy and responsiveness to treatment suggest that manual dexterity may represent a useful clinical marker in schizophrenia.
在精神分裂症患者中,手部灵巧性受损是常见现象。然而,目前缺乏对导致灵巧性受损的关键感觉运动成分的定量描述。灵巧性的关键成分是否受到不同程度的影响,以及它们与临床特征之间的关系也尚不清楚。我们使用四项视觉运动任务,对35名病情稳定的精神分裂症患者和20名年龄匹配的对照受试者的灵巧程度进行了量化:(i)力跟踪以量化视觉运动精度;(ii)顺序手指敲击以测量运动序列记忆;(iii)单指敲击以评估时间规律性;(iv)多指敲击以测量手指运动的独立性。我们还进行了各种临床和神经心理学测试。一个患者亚组(n = 15)参加了为期14周的认知康复方案,并在康复前后接受了评估。与对照受试者相比,精神分裂症患者在力跟踪方面表现出更大的误差,敲击序列的记忆较差,敲击规律性降低,手指个体化程度降低。一项综合表现指标区分患者和对照的灵敏度为0.79,特异度为0.9。除了力跟踪误差外,没有其他灵巧性成分与抗精神病药物相关。在患者中,一些灵巧性成分与神经学软体征、阳性和阴性症状量表(PANSS)或神经心理学分数相关。这表明这些成分的认知贡献存在差异。认知康复导致PANSS、跟踪误差和序列记忆有显著改善(药物治疗无变化)。这些发现表明,感觉运动控制的多个方面导致了精神分裂症患者手部灵巧性受损。只有视觉运动精度与抗精神病药物有关。良好的诊断准确性和对治疗的反应性表明,手部灵巧性可能是精神分裂症中一个有用的临床指标。