Nakamura Shigeki, Miyazaki Taiga, Izumikawa Koichi, Kakeya Hiroshi, Saisho Yutaka, Yanagihara Katsunori, Miyazaki Yoshitsugu, Mukae Hiroshi, Kohno Shigeru
Department of Respiratory Diseases, Nagasaki University Hospital.
Department of Chemotherapy and Mycoses, National Institute of Infectious Diseases, Tokyo, Japan.
Open Forum Infect Dis. 2017 Jun 19;4(3):ofx129. doi: 10.1093/ofid/ofx129. eCollection 2017 Summer.
Clinical studies comparing the different neuraminidase inhibitors for treatment of at-risk patients with influenza have not been performed. To optimize such treatments, we assessed the efficacy and safety of intravenous peramivir compared with oral oseltamivir in treating seasonal influenza A or B virus infection.
A multicenter, randomized, controlled clinical trial was conducted from December 2012 to May 2014 in high-risk patients infected with seasonal influenza. A total of 92 adult inpatients and outpatients with high risk factors (HRFs) were treated by either a single intravenous infusion of peramivir (600 mg) or oral administration of oseltamivir (75 mg, twice per day for 5 days).
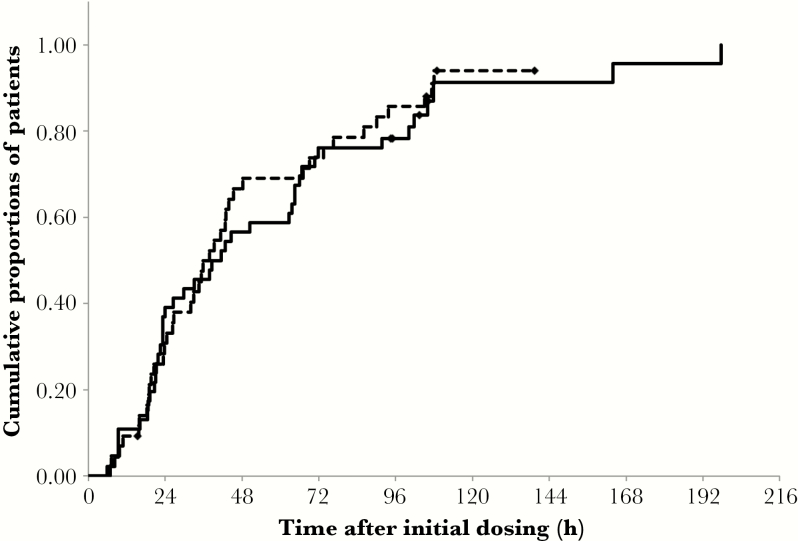
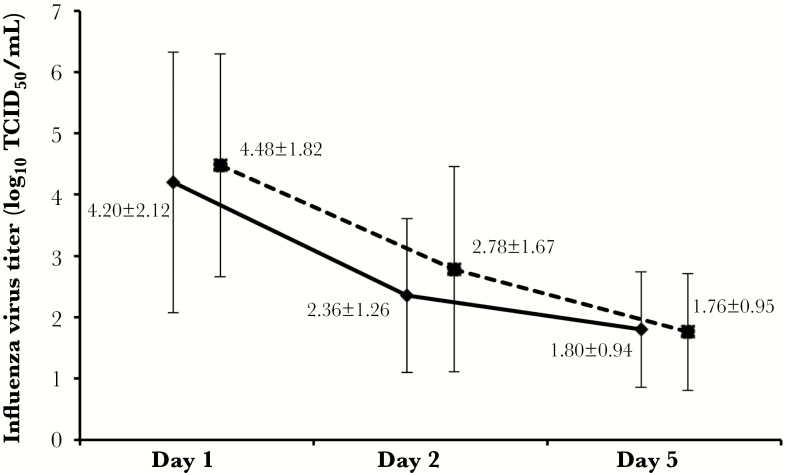
The median times to clinical stability (time to reach <37°C) were 40.0 hours (95% confidence interval [CI] = 23.3-64.5) and 37.8 hours (95% CI = 26.3-45.3) in the peramivir and oseltamivir groups, respectively; these values did not reveal a significant difference. The virus titer and change of mean total symptom scores decreased similarly with both treatments. Results of step-wise regression suggested that virus type was a significantly effective prognostic factor with respect to illness resolution. Adverse events (AEs) with peramivir and oseltamivir occurred in 2.2% (n = 1/46) and 13.0% (n = 6/46) of patients, respectively. The severity of AEs was mild in all cases except 2 patients who showed pneumonia or COPD aggravation; both were in the oseltamivir group.
Intravenous peramivir was effective based on the result of direct comparison with oral oseltamivir. Thus our data show that peramivir is a useful option for the treatment of influenza-infected patients with HRFs.
尚未开展比较不同神经氨酸酶抑制剂治疗流感高危患者的临床研究。为优化此类治疗,我们评估了静脉注射帕拉米韦与口服奥司他韦治疗季节性甲型或乙型流感病毒感染的疗效和安全性。
2012年12月至2014年5月,在感染季节性流感的高危患者中开展了一项多中心、随机、对照临床试验。共有92例具有高危因素(HRF)的成年住院患者和门诊患者接受了单次静脉输注帕拉米韦(600 mg)或口服奥司他韦(75 mg,每日两次,共5天)治疗。
帕拉米韦组和奥司他韦组临床稳定(体温降至<37°C)的中位时间分别为40.0小时(95%置信区间[CI]=23.3-64.5)和37.8小时(95%CI=26.3-45.3);这些值未显示出显著差异。两种治疗方法下病毒滴度和平均总症状评分的变化相似。逐步回归结果表明,病毒类型是疾病缓解的一个显著有效预后因素。接受帕拉米韦和奥司他韦治疗的患者不良事件(AE)发生率分别为2.2%(n=1/46)和13.0%(n=6/46)。除2例出现肺炎或慢性阻塞性肺疾病(COPD)加重的患者外,所有AE的严重程度均为轻度;这2例患者均在奥司他韦组。
基于与口服奥司他韦的直接比较结果,静脉注射帕拉米韦是有效的。因此,我们的数据表明,帕拉米韦是治疗具有HRF的流感感染患者的一个有用选择。