International College of Medicine, Institute of Public Health, International Health Program, National Yang Ming University, Taipei, Taiwan, Republic of China.
University of Melbourne, Parkville, VIC, Australia.
Int J Equity Health. 2017 Aug 7;16(1):140. doi: 10.1186/s12939-017-0626-7.
Acute respiratory infections (ARI) are major causes of morbidity and mortality in many low-income countries. Although factors associated with ARI symptoms in children under 5 years of age have been identified; however, variation in their prevalence resulting from regional-specific proximate determinants has received little attention. Therefore, we aim to investigate the specific regional determinants of overall and wealth-related inequality in children having ARI in Nigeria over a decade.
We analyzed trends in development of ARI symptoms among children under 5 years of age in Nigeria using nationally representative cross sectional surveys carried out in 2003, 2008 and 2013. Overall- and household wealth index based- inequality in the distribution of prevalence of ARI symptoms were estimated by region using Gini index and Concentration Index, respectively. Multivariate logistic regressions for complex survey and decomposition analysis for both indexes were used to calculate percentual contribution.
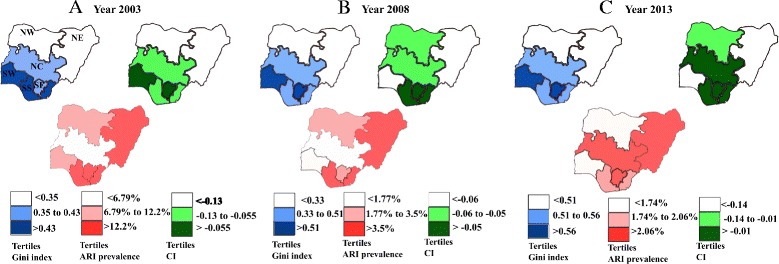
We found a decreasing trend in development of ARI symptoms over the decade between regions. Children in South Western region had reduced likelihood of developing the symptoms. Concentration index (CI) for the prevalence of ARI symptoms over the years and across regions had negative values (all p < 0.05). Gini index (GI) varies from 0.21 in North East to 0.62 in South Western region. Furthermore, the mapping showed that the extent at which both inequalities contribute to ARI symptoms prevalence in each region is different. The four major sources of wealth-related inequalities were poor households, no maternal education, biomass cooking, and rural area. The major contributors to overall inequalities were having a child aged 6 to 23 months, having no maternal education, having no vaccination card, and having a high birth order/short birth interval.
Although ARI prevalence decreased over the decade, it has remained unequally distributed between regions and over the time. The sources of those inequalities are context sensitive. Thus, in future health promotion initiatives, it is imperative to account for regional variations in the distribution of ARI.
急性呼吸道感染(ARI)是许多低收入国家发病率和死亡率的主要原因。虽然已经确定了与 5 岁以下儿童 ARI 症状相关的因素;然而,由于区域特定的近因,其患病率的差异受到的关注较少。因此,我们旨在调查过去十年中尼日利亚儿童 ARI 的总体和与财富相关的不平等的具体区域决定因素。
我们使用 2003 年、2008 年和 2013 年进行的全国代表性横断面调查,分析了尼日利亚 5 岁以下儿童急性呼吸道感染症状的发展趋势。使用基尼指数和集中指数分别按地区估算 ARI 症状流行率的总体和家庭财富指数为基础的不平等。使用多变量复杂调查逻辑回归和两个指数的分解分析来计算百分比贡献。
我们发现过去十年间,各地区急性呼吸道感染症状的发展呈下降趋势。西南部地区的儿童患该病的可能性较低。多年来,各地区急性呼吸道感染症状的患病率集中指数(CI)均为负值(均<0.05)。基尼指数(GI)在东北区为 0.21,在西南区为 0.62。此外,映射结果显示,这两种不平等对每个地区 ARI 症状流行程度的贡献程度不同。与财富相关的不平等的四个主要来源是贫困家庭、母亲没有受过教育、生物质烹饪和农村地区。导致总体不平等的主要因素是孩子年龄在 6 至 23 个月、母亲没有受过教育、没有疫苗接种卡和出生顺序较高/出生间隔较短。
尽管过去十年中 ARI 的患病率有所下降,但在各地区之间和时间上仍然存在不平等分布。这些不平等的根源是与具体情况相关的。因此,在未来的健康促进倡议中,必须考虑 ARI 分布的区域差异。