Jackson Michael L, Chung Jessie R, Jackson Lisa A, Phillips C Hallie, Benoit Joyce, Monto Arnold S, Martin Emily T, Belongia Edward A, McLean Huong Q, Gaglani Manjusha, Murthy Kempapura, Zimmerman Richard, Nowalk Mary P, Fry Alicia M, Flannery Brendan
From the Group Health Research Institute (now Kaiser Permanente Washington Health Research Institute), Seattle (M.L.J., L.A.J., C.H.P., J.B.); Centers for Disease Control and Prevention, Atlanta (J.R.C., A.M.F., B.F.); University of Michigan, Ann Arbor (A.S.M., E.T.M.); Marshfield Clinic Research Foundation, Marshfield WI (E.A.B., H.Q.M.); Baylor Scott and White Health, Texas A&M College of Medicine, Temple (M.G., K.M.); and University of Pittsburgh, Pittsburgh (R.Z., M.P.N.).
N Engl J Med. 2017 Aug 10;377(6):534-543. doi: 10.1056/NEJMoa1700153.
The A(H1N1)pdm09 virus strain used in the live attenuated influenza vaccine was changed for the 2015-2016 influenza season because of its lack of effectiveness in young children in 2013-2014. The Influenza Vaccine Effectiveness Network evaluated the effect of this change as part of its estimates of influenza vaccine effectiveness in 2015-2016.
We enrolled patients 6 months of age or older who presented with acute respiratory illness at ambulatory care clinics in geographically diverse U.S. sites. Using a test-negative design, we estimated vaccine effectiveness as (1-OR)×100, in which OR is the odds ratio for testing positive for influenza virus among vaccinated versus unvaccinated participants. Separate estimates were calculated for the inactivated vaccines and the live attenuated vaccine.
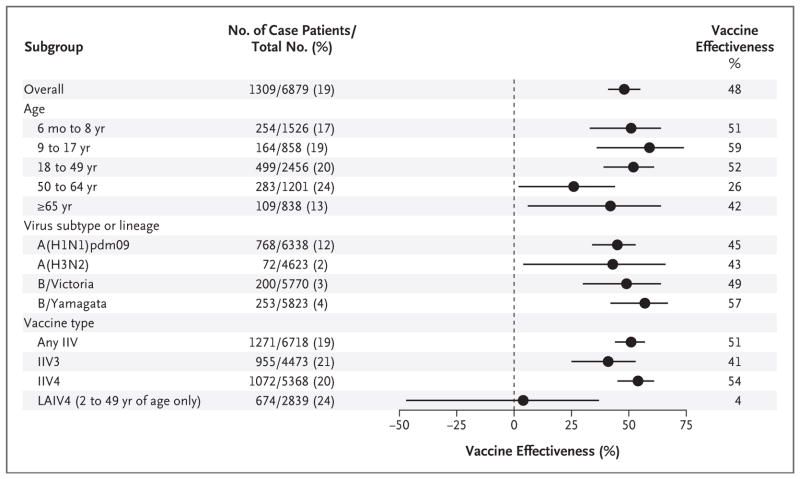
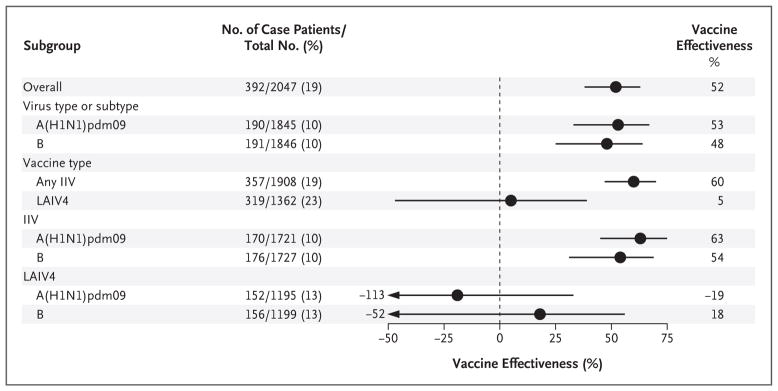
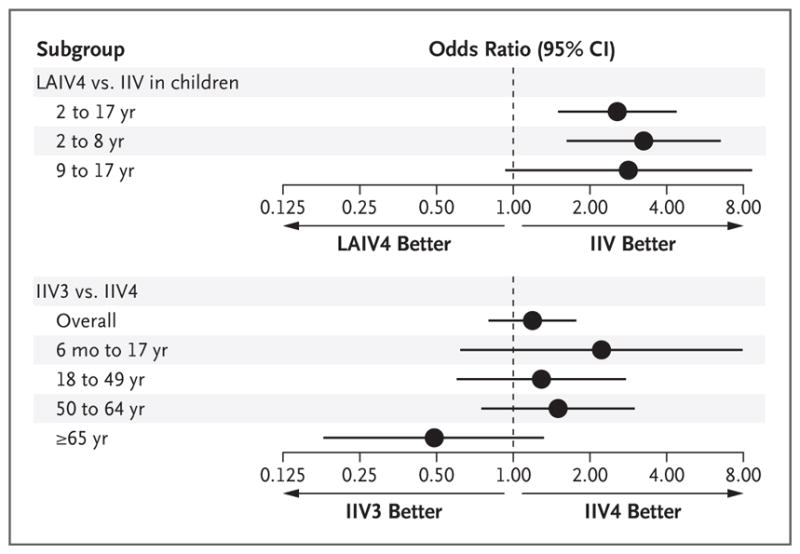
Among 6879 eligible participants, 1309 (19%) tested positive for influenza virus, predominantly for A(H1N1)pdm09 (11%) and influenza B (7%). The effectiveness of the influenza vaccine against any influenza illness was 48% (95% confidence interval [CI], 41 to 55; P<0.001). Among children 2 to 17 years of age, the inactivated influenza vaccine was 60% effective (95% CI, 47 to 70; P<0.001), and the live attenuated vaccine was not observed to be effective (vaccine effectiveness, 5%; 95% CI, -47 to 39; P=0.80). Vaccine effectiveness against A(H1N1)pdm09 among children was 63% (95% CI, 45 to 75; P<0.001) for the inactivated vaccine, as compared with -19% (95% CI, -113 to 33; P=0.55) for the live attenuated vaccine.
Influenza vaccines reduced the risk of influenza illness in 2015-2016. However, the live attenuated vaccine was found to be ineffective among children in a year with substantial inactivated vaccine effectiveness. Because the 2016-2017 A(H1N1)pdm09 strain used in the live attenuated vaccine was unchanged from 2015-2016, the Advisory Committee on Immunization Practices made an interim recommendation not to use the live attenuated influenza vaccine for the 2016-2017 influenza season. (Funded by the Centers for Disease Control and Prevention and the National Institutes of Health.).
由于2013 - 2014年甲型H1N1流感减毒活疫苗(LAIV)中所使用的甲型H1N1pdm09病毒株对幼儿缺乏有效性,因此在2015 - 2016年流感季节对其进行了更换。流感疫苗效力网络评估了这一变化的影响,作为其对2015 - 2016年流感疫苗效力估计的一部分。
我们纳入了年龄在6个月及以上、在美国不同地理位置的门诊诊所出现急性呼吸道疾病的患者。采用检测阴性设计,我们将疫苗效力估计为(1 - OR)×100,其中OR是接种疫苗与未接种疫苗参与者中流感病毒检测呈阳性的比值比。分别计算了灭活疫苗和减毒活疫苗的效力估计值。
在6879名符合条件的参与者中,1309人(19%)流感病毒检测呈阳性,主要为甲型H1N1pdm09(11%)和乙型流感(7%)。流感疫苗对任何流感疾病的效力为48%(95%置信区间[CI],41至55;P<0.001)。在2至17岁的儿童中,灭活流感疫苗的效力为60%(95%CI,47至70;P<0.001),而未观察到减毒活疫苗有效(疫苗效力为5%;95%CI, - 47至39;P = 0.80)。对于灭活疫苗,儿童中针对甲型H1N1pdm09的疫苗效力为63%(95%CI,45至75;P<0.001),而减毒活疫苗为 - 19%(95%CI, - 113至33;P = 0.55)。
流感疫苗在2015 - 2016年降低了流感疾病的风险。然而,在灭活疫苗效力显著的一年中,发现减毒活疫苗在儿童中无效。由于2016 - 2017年减毒活疫苗中所使用的甲型H1N1pdm09毒株与2015 - 2016年相同,免疫实践咨询委员会做出了一项临时建议,即在2016 - 2017年流感季节不使用减毒活流感疫苗。(由疾病控制和预防中心及国立卫生研究院资助。)