Haynes-Maslow Lindsey, Leone Lucia A
Department of Agricultural and Human Sciences, School of Public Health and Health Professions North Carolina State University, 512 Brickhaven Drive, Suite 240, Campus Box 7606, Raleigh, NC, 27695, USA.
Department of Community Health and Health Behavior, School of Public Health and Health Professions, University at Buffalo, Buffalo, NY, USA.
BMC Public Health. 2017 Aug 9;17(1):648. doi: 10.1186/s12889-017-4658-0.
Inequitable access to healthy food may contribute to health disparities. This study examines the relationship between the prevalence of adult diabetes and food access in the U.S. by county economic/racial composition.
An ecological study from 2012 was used to estimate the relationship between diabetes and retail food outlet access. County diabetes prevalence was measured based on individual responses to the Behavioral Risk Factor Surveillance Survey question, "Have you ever been told by a doctor that you have diabetes?" If the answer was "yes" individuals were classified as having diabetes. Retail food outlets included grocery stores, supercenters, farmer's markets, full-service restaurants, fast food restaurants and convenience stores. Counties were categorized as "high-poverty" or "low-poverty". Counties were categorized as low (< 4.6%), medium (4.6%-31.0%), and high (> 31.0%) percent minority residents. Multiple linear regression models estimated the association between retail food outlets and diabetes, controlling for confounders, and testing for interactions between retail food outlets and county racial composition. Regression models were conditioned on county economic composition. Data were analyzed in 2016.
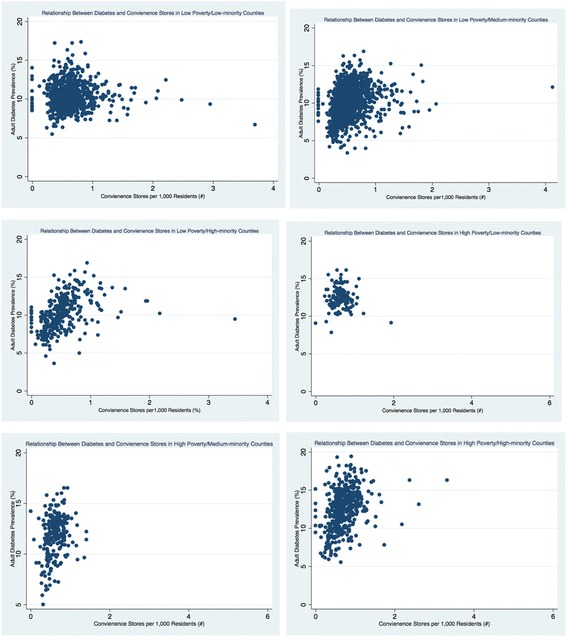
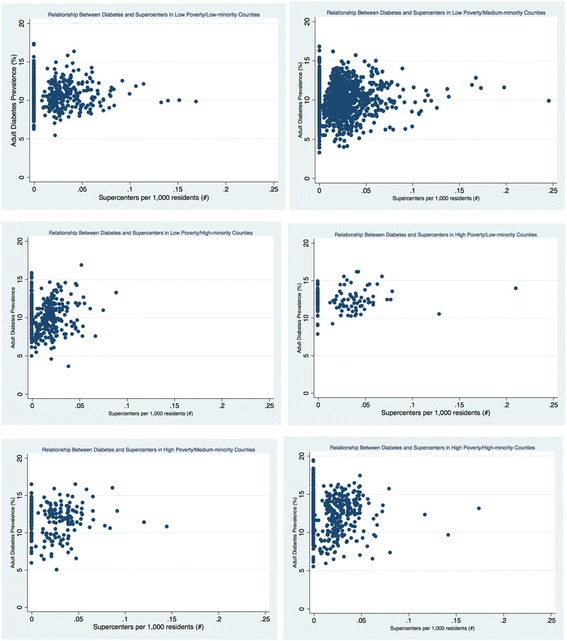
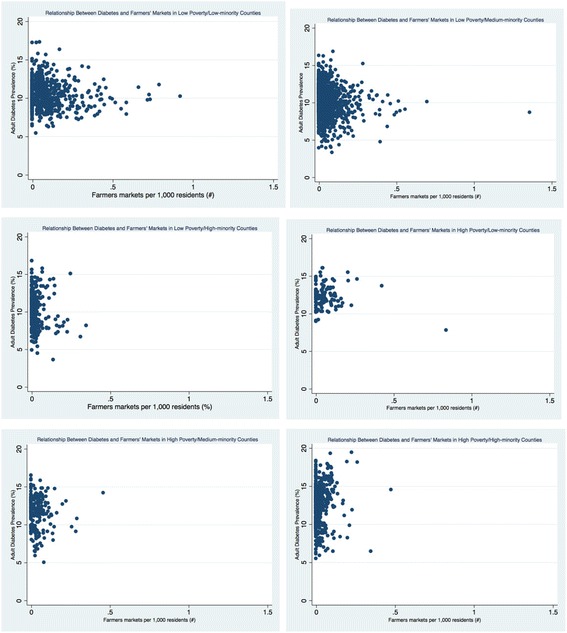
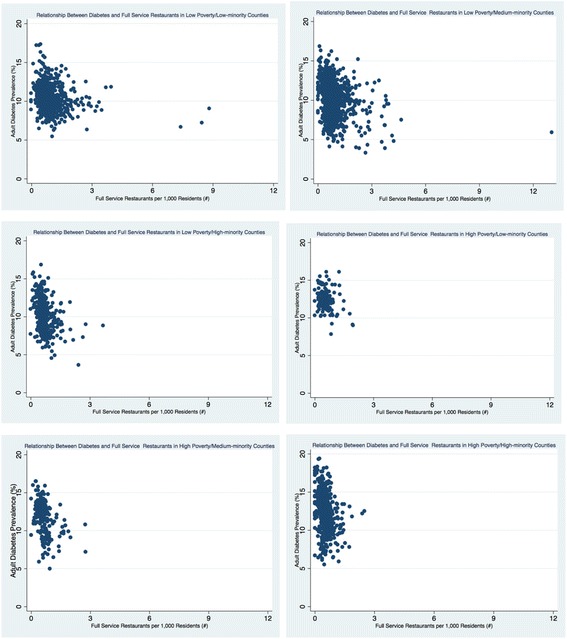
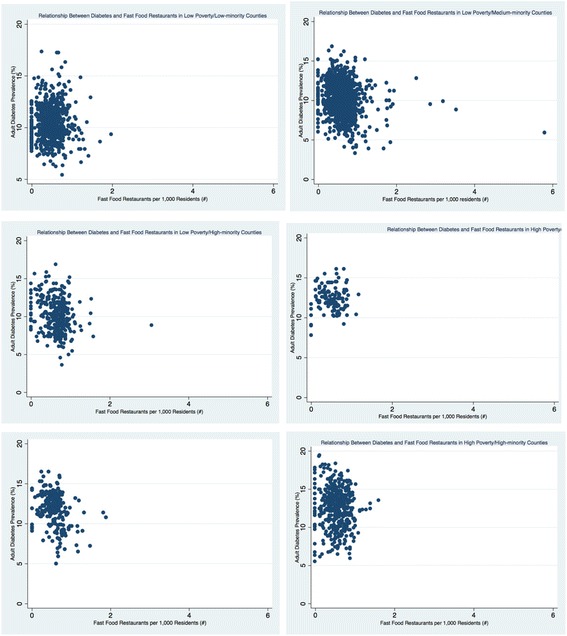
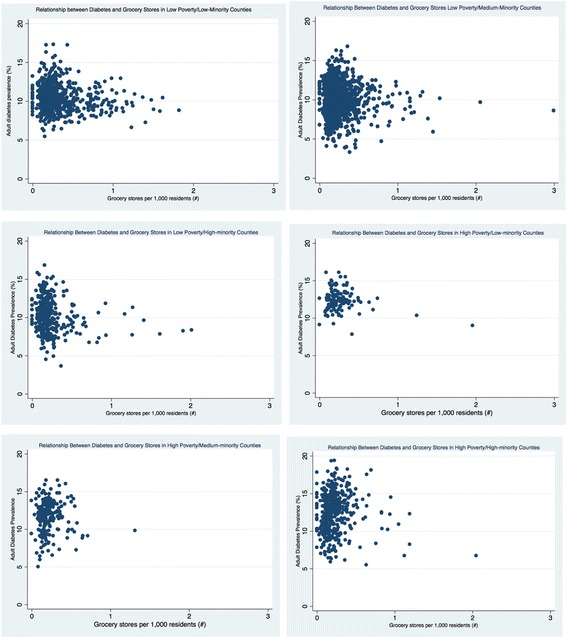
Density of retail foods outlets varied greatly by county economic and racial composition; counties with medium-minority populations had the least access to grocery stores and the highest access to fast food restaurants and convenience stores. Low poverty/low-minority population counties had the greatest access to farmer's markets and grocery stores. For low poverty/low-minority counties, grocery stores were associated with decreased of diabetes prevalence. Supercenters were associated with an increase in diabetes prevalence for high-poverty/low-minority counties. Only low poverty/medium-minority counties had a statistically significant relationship between farmer's markets and diabetes prevalence. Fast food restaurants were found to be positively associated with diabetes prevalence in all counties except high poverty/medium-minority. However, only low poverty/low-minority counties had a statistically significant relationship. Across all models, access to full service restaurants were significantly associated with lower prevalence of diabetes. Generally, access to convenience stores were associated with increased diabetes prevalence, except for high poverty/low-minority counties.
The food environment is more strongly associated with diabetes prevalence for wealthier counties with a lower proportion of minority residents. This is important given efforts to increase food access in vulnerable communities. Availability of healthier food may not be enough to change health outcomes.
获得健康食品的机会不平等可能导致健康差距。本研究按县的经济/种族构成考察了美国成人糖尿病患病率与食品可及性之间的关系。
采用一项2012年的生态学研究来估计糖尿病与零售食品店可及性之间的关系。县糖尿病患病率是根据个人对行为危险因素监测调查问题“你是否曾被医生告知患有糖尿病?”的回答来衡量的。如果回答为“是”,则该个体被归类为患有糖尿病。零售食品店包括杂货店、大型超市、农贸市场、提供全方位服务的餐厅、快餐店和便利店。县被分为“高贫困”或“低贫困”。县被分为少数族裔居民比例低(<4.6%)、中等(4.6%-31.0%)和高(>31.0%)的类别。多元线性回归模型估计了零售食品店与糖尿病之间的关联,控制了混杂因素,并检验了零售食品店与县种族构成之间的相互作用。回归模型以县的经济构成作为条件。数据于2016年进行分析。
零售食品店的密度因县的经济和种族构成而有很大差异;少数族裔人口中等的县获得杂货店的机会最少,获得快餐店和便利店的机会最多。低贫困/少数族裔人口少的县获得农贸市场和杂货店的机会最大。对于低贫困/少数族裔人口少的县,杂货店与糖尿病患病率降低有关。对于高贫困/少数族裔人口少的县,大型超市与糖尿病患病率增加有关。只有低贫困/少数族裔人口中等的县,农贸市场与糖尿病患病率之间存在统计学上的显著关系。除了高贫困/少数族裔人口中等的县外,在所有县中,快餐店与糖尿病患病率呈正相关。然而,只有低贫困/少数族裔人口少的县存在统计学上的显著关系。在所有模型中,获得提供全方位服务的餐厅与糖尿病患病率较低显著相关。一般来说,获得便利店与糖尿病患病率增加有关,但高贫困/少数族裔人口少的县除外。
对于少数族裔居民比例较低的富裕县,食品环境与糖尿病患病率的关联更为密切。鉴于在弱势社区增加食品可及性的努力,这一点很重要。提供更健康的食品可能不足以改变健康结果。