Centre for Population Health Research, Sansom Institute for Health Research, University of South Australia, Adelaide, Australia.
South Australian Prostate Cancer Clinical Outcomes Collaborative, Repatriation General Hospital, Adelaide, Australia.
BMC Cancer. 2017 Aug 10;17(1):537. doi: 10.1186/s12885-017-3533-9.
A new 5-tiered grading grouping system has recently been endorsed for reporting of prostate cancer (PCa) grade to better reflect escalating risk of progression and cancer death. While several validations of the new grade groupings have been undertaken, most have involved centralised pathological review by specialist urological pathologists.
Participants included 4268 men with non-metastatic PCa diagnosed between 2006 and 2013 from the multi-institutional South Australia Prostate Cancer Clinical Outcomes Collaborative registry. PCa-specific survival and biochemical recurrence-free survival were compared across the five grade groups using multivariable competing risk regression.
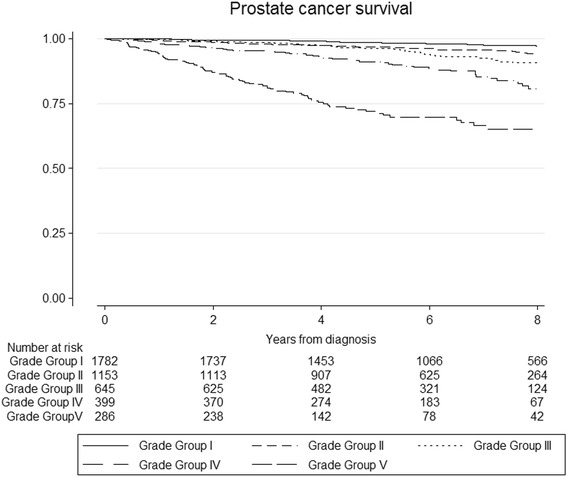
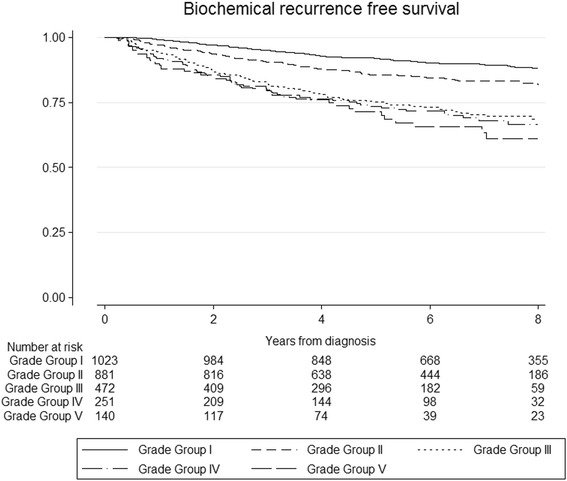
For the entire cohort, risk of PCa death increased with increasing grade groups (at biopsy) Adjusted subdistribution-hazard ratios [sHR] and 95% confidence intervals [95%CI] were: 2.2 (1.5-3.6); 2.5 (1.6-4.2); 4.1 (2.6-6.7) and 8.7 (4.5-14.0) for grade groups II (pattern 3 + 4), III (pattern 4 + 3), IV (total score 8) and V (total score 9-10) respectively, relative to grade group I (total score < =6). Clear gradients in risk of PCa death were observed for radical prostatectomy (RP), but were less clear for those who had radiotherapy (RT) with curative intent and those who were managed conservatively. Likewise, risk of biochemical recurrence increased across grade groups, with a strong and clear gradient for men undergoing RP [sHR (95%CI): 2.0 (1.4-2.8); 3.8 (2.9-5.9); 5.3 (3.5-8.0); 11.2 (6.5-19.2) for grade groups II, III, IV and V respectively, relative to grade group I], and a less clear gradient for men undergoing RT.
In general, the new five-tiered grade groupings distinguished PCa survival and recurrence outcomes for men with PCa. The absence of a clear gradient for RT may be due to heterogeneity in this patient group.
最近,一种新的 5 级分组系统已被认可用于前列腺癌 (PCa) 分级报告,以更好地反映进展和癌症死亡的风险增加。虽然已经对新的分级分组进行了多次验证,但大多数都涉及由泌尿科病理学家进行的集中病理审查。
参与者包括来自多机构南澳大利亚前列腺癌临床结果协作注册中心的 4268 名在 2006 年至 2013 年间诊断为非转移性 PCa 的男性。使用多变量竞争风险回归比较五个分级组的 PCa 特异性生存和生化无复发生存率。
在整个队列中,随着分级组的增加,PCa 死亡风险增加(在活检时)。调整后的亚分布风险比 [sHR] 和 95%置信区间 [95%CI] 为:2.2(1.5-3.6);2.5(1.6-4.2);4.1(2.6-6.7)和 8.7(4.5-14.0),分别用于分级组 II(模式 3+4)、III(模式 4+3)、IV(总评分 8)和 V(总评分 9-10),与分级组 I(总评分 <=6)相比。在接受根治性前列腺切除术 (RP) 的患者中观察到 PCa 死亡风险的明显梯度,但在接受有治愈意图的放疗 (RT) 且保守治疗的患者中则不太明显。同样,生化复发风险随分级组增加,接受 RP 的男性风险增加明显且呈梯度增加 [sHR(95%CI):2.0(1.4-2.8);3.8(2.9-5.9);5.3(3.5-8.0);11.2(6.5-19.2),分别用于分级组 II、III、IV 和 V,与分级组 I 相比],而接受 RT 的男性风险增加则不太明显。
总的来说,新的 5 级分级分组区分了 PCa 生存和复发结果。RT 中没有明显的梯度可能是由于该患者群体的异质性。