Miller Leanne K, Jerosch-Herold Christina, Shepstone Lee
School of Health Sciences, University of East Anglia, Norwich, Norfolk, United Kingdom.
School of Health Sciences, University of East Anglia, Norwich, Norfolk, United Kingdom.
J Hand Ther. 2017 Oct-Dec;30(4):432-446. doi: 10.1016/j.jht.2017.05.011. Epub 2017 Aug 12.
Systematic review.
Prolonged hand edema can have detrimental effects on range of motion and function. There is no consensus on how best to manage traumatic subacute edema. This is the first systematic review which examines the clinical effectiveness of edema treatments on hand volume.
The purpose of this systematic review was to examine the evidence of effectiveness of treatments for sub-acute hand edema.
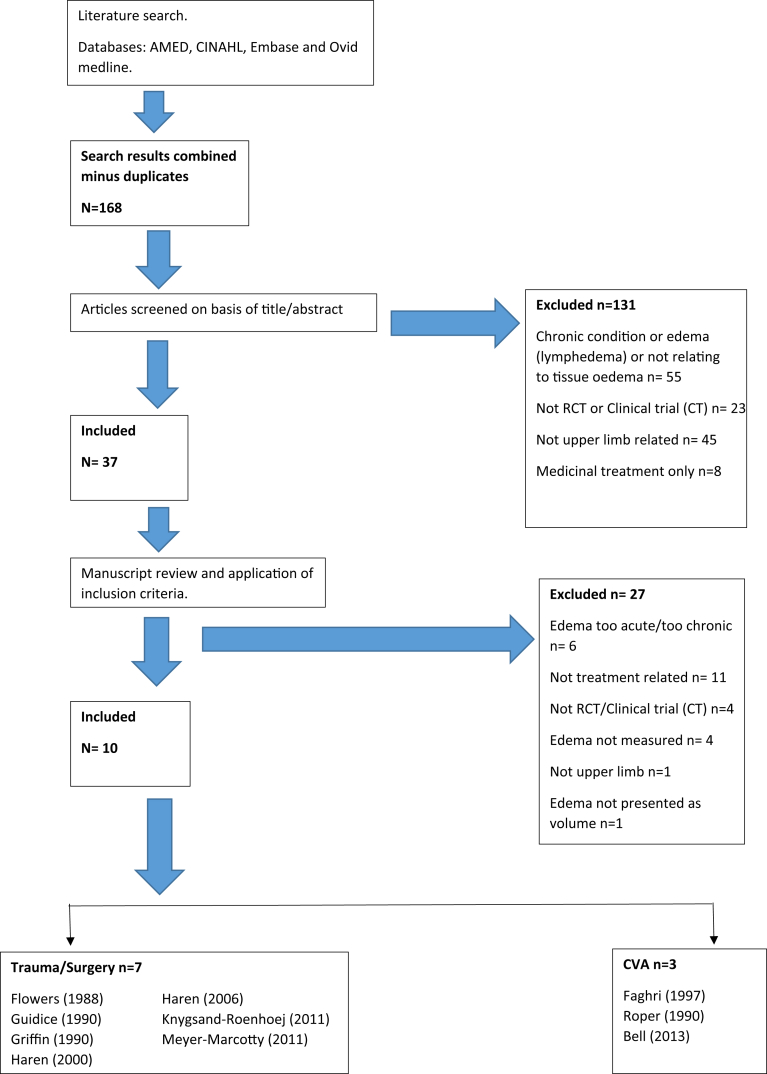
A literature search of AMED, CINAHL, Embase, and OVID MEDLINE (from inception to August 2015) was undertaken. Studies were selected if they met the following inclusion criteria: randomized controlled or controlled trials in adults who have subacute swelling after a recent upper limb musculoskeletal trauma or cerebral vascular attack or after surgery. Two independent assessors rated study quality and risk of bias using the 24-point MacDermid Structured Effectiveness Quality Evaluation Scale (SEQES).
Ten studies met the inclusion criteria. Study quality ranged from 23 to 41 out of 48 points on the SEQES. A total of 16 edema interventions were evaluated across the studies. Due to heterogeneity of the patient characteristics, interventions, and outcomes assessed, it was not possible to pool the results from all studies. Therefore, a narrative best evidence synthesis was undertaken. There is low to moderate quality evidence with limited confidence in the effect estimate to support the use of manual edema mobilization methods in conjunction with standard therapy to reduce problematic hand edema.
Manual edema mobilization techniques should be considered in conjunction with conventional therapies, in cases of excessive edema or when the edema has not responded to conventional treatment alone; however, manual edema mobilization is not advocated as a routine intervention.
2b.
系统评价。
手部长期水肿会对活动范围和功能产生不利影响。对于如何最佳处理创伤性亚急性水肿尚无共识。这是第一项研究水肿治疗对手部体积临床疗效的系统评价。
本系统评价的目的是检验亚急性手部水肿治疗有效性的证据。
检索了AMED、CINAHL、Embase和OVID MEDLINE(从创刊至2015年8月)。如果研究符合以下纳入标准则被选中:针对近期上肢肌肉骨骼创伤、脑血管意外或手术后出现亚急性肿胀的成年人进行的随机对照试验或对照试验。两名独立评估者使用24分的麦克德米德结构化有效性质量评估量表(SEQES)对研究质量和偏倚风险进行评分。
10项研究符合纳入标准。SEQES评分中研究质量范围为23至41分(满分48分)。各项研究共评估了16种水肿干预措施。由于患者特征、干预措施和评估结果的异质性,无法汇总所有研究的结果。因此,进行了叙述性最佳证据综合分析。有低至中等质量的证据,对效应估计的信心有限,支持将手法水肿松动方法与标准治疗联合使用以减轻手部严重水肿。
对于水肿过度或水肿对单纯常规治疗无反应的情况,应考虑将手法水肿松动技术与传统疗法联合使用;然而,不主张将手法水肿松动作为常规干预措施。
2b。