Farach-Carson Mary C, Lin Sue-Hwa, Nalty Theresa, Satcher Robert L
Department of Diagnostic and Biomedical Sciences, School of Dentistry, The University of Texas Health Science Center at Houston, Houston, TX, United States.
Department of Translational Molecular Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
Front Oncol. 2017 Aug 7;7:163. doi: 10.3389/fonc.2017.00163. eCollection 2017.
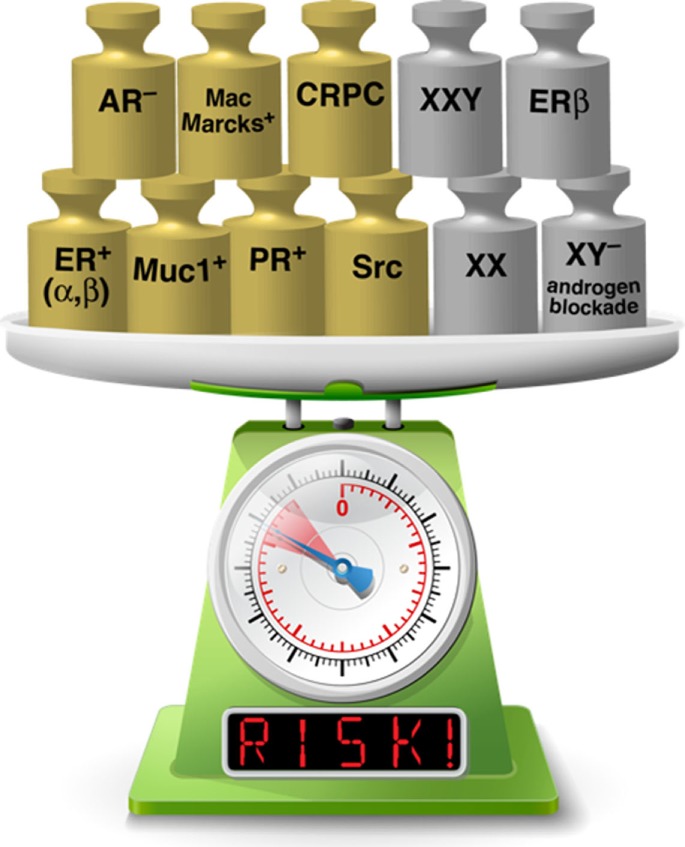
Sex-associated differences in bone metastasis formation from breast, lung, and prostate cancer exist in clinical studies, but have not been systematically reviewed. Differences in the bone marrow niche can be attributed to sexual dimorphism, to genetic variations that affect sex hormone levels, or to the direct effects of sex hormones, natural or exogenously delivered. This review describes the present understanding of sex-associated and sex hormone level differences in the marrow niche and in formation of bone metastasis during the transition of these three cancers from treatable disease to an often untreatable, lethal metastatic one. Our purpose is to provide insight into some underlying molecular mechanisms for hormonal influence in bone metastasis formation, and to the potential influence of sexual dimorphism, genetic differences affecting sex assignment, and sex hormone level differences on the bone niche and its favorability for metastasis formation. We reviewed publications in PubMed and EMBASE, including full length manuscripts, case reports, and clinical studies of relevance to our topic. We focused on bone metastasis formation in breast, lung, and prostate cancer because all three commonly present with bone metastases. Several clear observations emerged. For breast cancer bone metastasis formation, estrogen receptor (ER) signaling pathways indicate a role for ER beta (ERβ). Estrogen influences the bone microenvironment, creating and conditioning a favorable niche for colonization and breast cancer progression. For lung cancer, studies support the hypothesis that females have a more favorable bone microenvironment for metastasis formation. For prostate cancer, a decrease in the relative androgen to estrogen balance or a "feminization" of bone marrow favors bone metastasis formation, with a potentially important role for ERβ that may be similar to that in breast cancer. Long-term estrogen administration or androgen blockade in males may feminize the bone marrow niche to one more favorable for bone metastases in prostate cancer. Administration of androgens in females, especially combined with mastectomy, may reduce risk of developing bone metastatic breast cancer. We conclude that it should be considered that females, those with female-leaning genetic variations, or hormonal states that feminize the bone marrow, may offer favorable sites for bone metastases.
临床研究表明,乳腺癌、肺癌和前列腺癌在骨转移形成方面存在性别差异,但尚未进行系统综述。骨髓微环境的差异可归因于性二态性、影响性激素水平的基因变异,或性激素(天然的或外源性给予的)的直接作用。本综述描述了目前对骨髓微环境中与性别相关及性激素水平差异的理解,以及这三种癌症从可治疗疾病转变为通常无法治疗的致命转移性疾病过程中骨转移形成的情况。我们的目的是深入了解激素影响骨转移形成的一些潜在分子机制,以及性二态性、影响性别的基因差异和性激素水平差异对骨微环境及其对转移形成的适宜性的潜在影响。我们检索了PubMed和EMBASE上的出版物,包括与我们主题相关的全文手稿、病例报告和临床研究。我们重点关注乳腺癌、肺癌和前列腺癌的骨转移形成,因为这三种癌症都常出现骨转移。出现了几个明确的观察结果。对于乳腺癌骨转移的形成,雌激素受体(ER)信号通路表明雌激素受体β(ERβ)发挥作用。雌激素影响骨微环境,为肿瘤定植和乳腺癌进展创造并调节适宜的微环境。对于肺癌,研究支持这样的假设,即女性具有更有利于转移形成的骨微环境。对于前列腺癌,相对雄激素与雌激素平衡的降低或骨髓的“女性化”有利于骨转移的形成,ERβ可能发挥与乳腺癌中类似的潜在重要作用。男性长期给予雌激素或雄激素阻断可能使骨髓微环境女性化,使其对前列腺癌骨转移更有利。女性给予雄激素,尤其是联合乳房切除术,可能降低发生骨转移性乳腺癌的风险。我们得出结论,应考虑到女性、具有倾向女性的基因变异者或使骨髓女性化的激素状态,可能为骨转移提供适宜的部位。