Bettinger Lynne N, Waters Linda M, Reese Stephen W, Kutner Susan E, Jacobs Daniel I
Boston University Medical School, Boston, Mass.; Department of Surgery, Stanford University Medical Center, Stanford University School Stanford University Medical Center, Stanford School of Medicine, Stanford, Calif.; Department of Surgery Kaiser Permanente Medical Center San Jose, San Jose, Calif.; Adjunct Clinical Faculty, Division of Plastic Surgery, Department of Surgery, Stanford University, Stanford, Calif.; Columbia University, School of Professional Studies, Graduate Studies in Bioethics, New York, N.Y.; Department of Surgery, Brigham and Women's Hospital, Harvard Medical School, Boston, Mass.
Plast Reconstr Surg Glob Open. 2017 Jul 26;5(7):e1433. doi: 10.1097/GOX.0000000000001433. eCollection 2017 Jul.
Prepectoral breast reconstruction is increasingly popular. This study compares complications between 2 subpectoral and 1 prepectoral breast reconstruction technique.
Between 2008 and 2015, 294 two-staged expander breast reconstructions in 213 patients were performed with 1 of 3 surgical techniques: (1) Prepectoral, (2) subpectoral with acellular dermal matrix (ADM) sling ("Classic"), or (3) subpectoral/subserratus expander placement without ADM ("No ADM"). Demographics, comorbidities, radiation therapy, and chemotherapy were assessed for correlation with Clavien IIIb score outcomes. Follow-up was a minimum of 6 months.
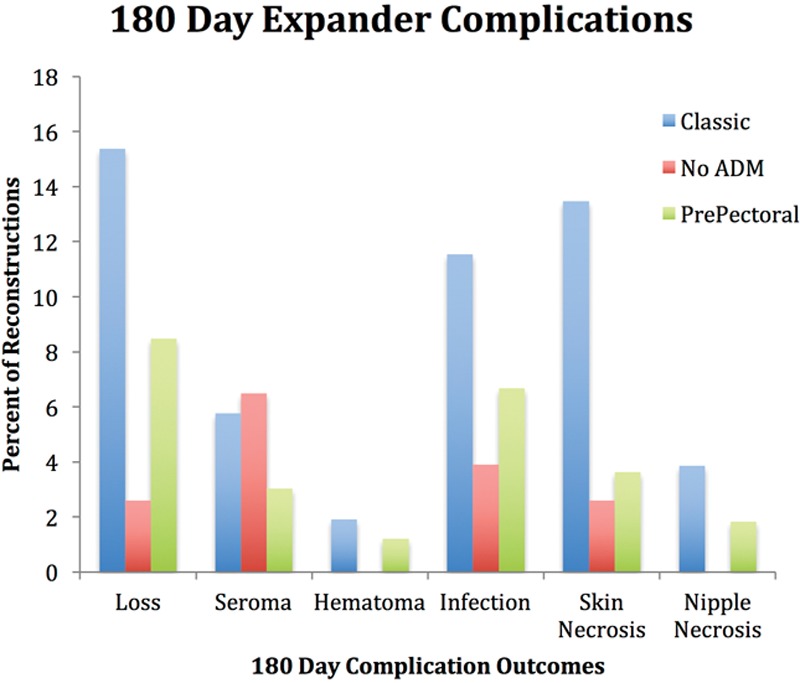
Surgical cohorts (n = 165 Prepectoral; n = 77 Classic; n = 52 No ADM) had comparable demographics except Classic had more cardiac disease ( = 0.03), No ADM had higher body mass index (BMI) ( = 0.01), and the Prepectoral group had more nipple-sparing mastectomies ( < 0.001). Univariate analysis showed higher expander complications with BMI ≥ 40 ( = 0.05), stage 4 breast cancer ( = 0.01), and contralateral prophylactic mastectomy ( = 0.1), whereas implant complications were associated with prior history of radiation ( < 0.01). There was more skin necrosis ( = 0.05) and overall expander complications ( = 0.01) in the Classic cohort, whereas the No ADM group trended toward the lowest expander complications among the 3. Multivariate analysis showed no difference in overall expander complication rates between the 3 groups matching demographics, mastectomy surgery, risks, and surgical technique.
Prepectoral and subpectoral Classic and No ADM breast reconstructions demonstrated comparable grade IIIb Clavien score complications. BMI > 40, stage 4 cancer, and contralateral prophylactic mastectomy were associated with adverse expander outcomes and a prior history of radiation therapy adversely impacted implant outcomes. Ninety-day follow-up for expander and implant complications may be a better National Surgical Quality Improvement Program measure.
胸肌前乳房重建越来越受欢迎。本研究比较了两种胸肌下和一种胸肌前乳房重建技术的并发症。
2008年至2015年期间,对213例患者进行了294例两阶段扩张器乳房重建,采用三种手术技术之一:(1)胸肌前,(2)胸肌下带脱细胞真皮基质(ADM)吊带(“经典法”),或(3)胸肌下/锯肌下放置扩张器且无ADM(“无ADM法”)。评估人口统计学、合并症、放疗和化疗与Clavien IIIb评分结果的相关性。随访至少6个月。
手术队列(胸肌前组n = 165;经典法组n = 77;无ADM法组n = 52)的人口统计学特征具有可比性,只是经典法组心脏病更多(P = 0.03),无ADM法组体重指数(BMI)更高(P = 0.01),且胸肌前组保乳手术更多(P < 0.001)。单因素分析显示,BMI≥40(P = 0.05)、IV期乳腺癌(P = 0.01)和对侧预防性乳房切除术(P = 0.1)时扩张器并发症更高,而植入物并发症与既往放疗史相关(P < 0.01)。经典法队列中皮肤坏死(P = 0.05)和总体扩张器并发症(P = 0.01)更多,而无ADM法组在三组中扩张器并发症趋向于最低。多因素分析显示,在匹配人口统计学、乳房切除术、风险和手术技术的情况下,三组之间总体扩张器并发症发生率无差异。
胸肌前、胸肌下经典法和无ADM法乳房重建的Clavien IIIb评分并发症相当。BMI>40、IV期癌症和对侧预防性乳房切除术与扩张器不良结局相关,既往放疗史对植入物结局有不利影响。对扩张器和植入物并发症进行90天随访可能是更好的国家外科质量改进计划指标。