Cintron Dahima, Lahr Brian D, Bailey Kent R, Santoro Nanette, Lloyd Robin, Manson JoAnn E, Neal-Perry Genevieve, Pal Lubna, Taylor Hugh S, Wharton Whitney, Naftolin Fredrick, Harman S Mitchell, Miller Virginia M
Mayo Clinic Graduate School, Mayo Clinic Rochester, MN.
Department of Health Sciences Research Division of Biomedical Statistics and Informatics, Mayo Clinic Rochester, MN.
Menopause. 2018 Feb;25(2):145-153. doi: 10.1097/GME.0000000000000971.
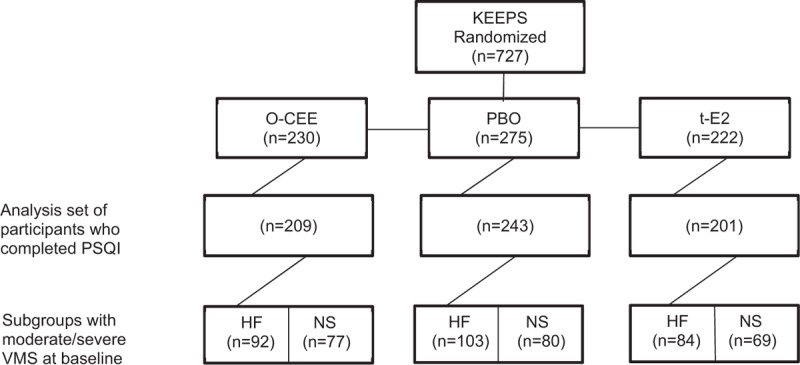
This study determined whether two different formulations of hormone therapy (HT): oral conjugated equine estrogens (o-CEE; 0.45 mg/d, n = 209), transdermal 17β-estradiol (t-E2; 50 μg/d, n = 201) plus cyclic progesterone (Prometrium, 200 mg) or placebo (PBO, n = 243) affected sleep domains in participants of the Kronos Early Estrogen Prevention Study.
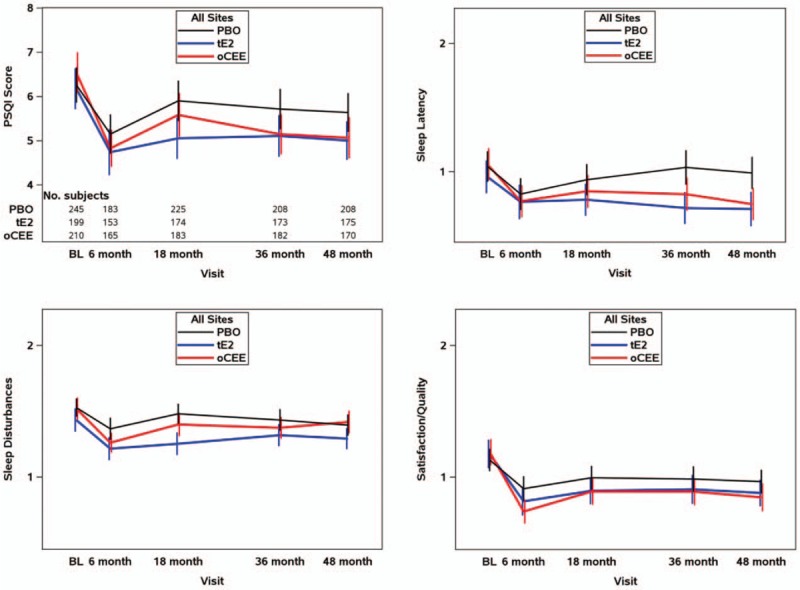
Participants completed the Pittsburgh Sleep Quality Index at baseline and during the intervention at 6, 18, 36, and 48 months. Global sleep quality and individual sleep domain scores were compared between treatments using analysis of covariance, and correlated with vasomotor symptom (VMS) scores using Spearman correlation coefficients.
Global Pittsburgh Sleep Quality Index scores (mean 6.3; 24% with score >8) were similar across groups at baseline and were reduced (improved sleep quality) by both HT (average change -1.27 [o-CEE] and -1.32 [t-E2]) when compared with PBO (-0.60; P = 0.001 [o-CEE vs PBO] and P = 0.002 [t-E2 vs PBO]). Domain scores for sleep satisfaction and latency improved with both HT. The domain score for sleep disturbances improved more with t-E2 than o-CEE or PBO. Global sleep scores significantly correlated with VMS severity (rs = 0.170, P < 0.001 for hot flashes; rs = 0.177, P < 0.001 for night sweats). Change in scores for all domains except sleep latency and sleep efficiency correlated with change in severity of VMS.
Poor sleep quality is common in recently menopausal women. Sleep quality improved with both HT formulations. The relationship of VMS with domains of sleep suggests that assessing severity of symptoms and domains of sleep may help direct therapy to improve sleep for postmenopausal women.
本研究确定了两种不同的激素疗法(HT)制剂:口服结合马雌激素(o-CEE;0.45毫克/天,n = 209)、经皮17β-雌二醇(t-E2;50微克/天,n = 201)加周期性黄体酮(普维拉,200毫克)或安慰剂(PBO,n = 243)对Kronos早期雌激素预防研究参与者睡眠领域的影响。
参与者在基线时以及干预期间的6、18、36和48个月完成匹兹堡睡眠质量指数评估。使用协方差分析比较各治疗组之间的总体睡眠质量和个体睡眠领域得分,并使用斯皮尔曼相关系数将其与血管舒缩症状(VMS)得分相关联。
基线时各组的匹兹堡睡眠质量指数总体得分(平均6.3;24%得分>8)相似,与PBO(-0.60;P = 0.001 [o-CEE与PBO比较]和P = 0.002 [t-E2与PBO比较])相比,两种HT制剂均使得分降低(睡眠质量改善)(平均变化-1.27 [o-CEE]和-1.32 [t-E2])。两种HT制剂均使睡眠满意度和入睡潜伏期领域得分得到改善。睡眠障碍领域得分的改善,t-E2比o-CEE或PBO更明显。总体睡眠得分与VMS严重程度显著相关(潮热:rs = 0.170,P < 0.001;盗汗:rs = 0.177,P < 0.001)。除入睡潜伏期和睡眠效率外,所有领域得分的变化均与VMS严重程度的变化相关。
睡眠质量差在近期绝经的女性中很常见。两种HT制剂均改善了睡眠质量。VMS与睡眠领域的关系表明,评估症状严重程度和睡眠领域可能有助于指导治疗,以改善绝经后女性的睡眠。