Haufe Annika, Leeners Brigitte
Department of Reproductive Endocrinology, University Hospital Zurich, University of Zurich, CH-8091 Zürich, Switzerland.
J Endocr Soc. 2023 Mar 15;7(5):bvad036. doi: 10.1210/jendso/bvad036. eCollection 2023 Mar 6.
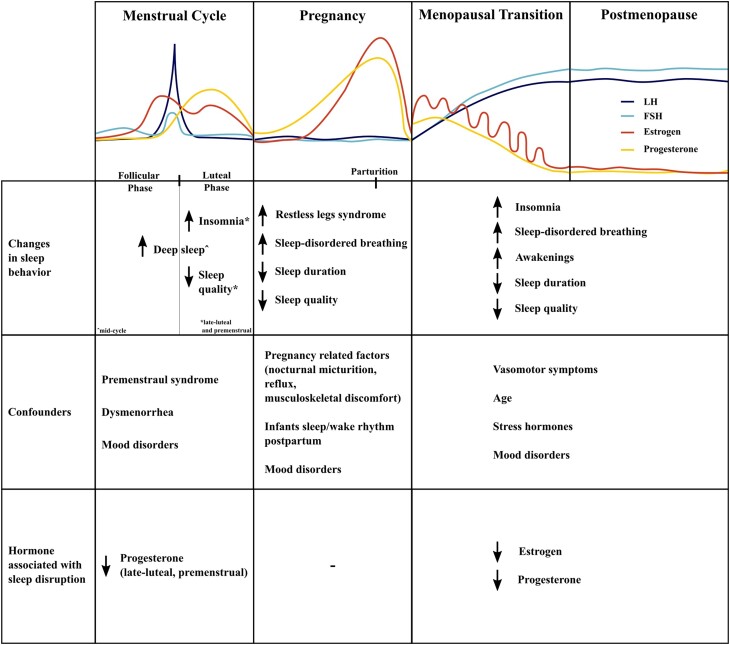
Fluctuations of reproductive hormones are associated with various forms of sleep disturbances and specific sleep disorders, such as insomnia or sleep-disordered breathing, across different stages of reproductive aging. During the menstrual cycle, sleep is particularly disrupted during the late luteal phase, as demonstrated by both objective and subjective measurements of sleep. Progesterone and its metabolites generally have sleep-promoting effects. A steep decline in progesterone, for example, during the late luteal phase, is associated with sleep disruption. Endogenous estrogen shows no clear correlation with sleep alterations in relation to the menstrual cycle. During pregnancy, sleep disruption is not associated with changes in estrogen or progesterone but rather with changing physiological factors, such as nocturnal micturition, gastroesophageal reflux, or musculoskeletal discomfort, all substantial factors that most likely mask any effect of hormones. Both endogenous and exogenous estrogen, as well as progesterone, are positively associated with sleep during the menopausal transition. A marked improvement of sleep disturbances is observed with perimenopausal hormone therapy. As this effect is not seen in younger women receiving contraceptive therapy, other causes of sleep disturbances, such as aging and related changes in metabolism of stress hormones, secondary effects of vasomotor symptoms, or depression, must be considered. Gonadotropins are less associated with sleep disturbances than ovarian hormones, except for during the menopausal transition where follicle-stimulating hormone is related to sleep disruption. Further, hyperandrogenism, as seen in women with polycystic ovary syndrome, is associated with sleep disturbances and specific sleep disorders, for example, obstructive sleep apnea.
在生殖衰老的不同阶段,生殖激素的波动与各种形式的睡眠障碍以及特定的睡眠疾病相关,如失眠或睡眠呼吸紊乱。在月经周期中,黄体后期睡眠尤其容易受到干扰,这已通过睡眠的客观和主观测量得到证实。孕酮及其代谢产物通常具有促进睡眠的作用。例如,在黄体后期孕酮的急剧下降与睡眠干扰有关。内源性雌激素与月经周期相关的睡眠改变没有明显的相关性。在怀孕期间,睡眠干扰与雌激素或孕酮的变化无关,而是与生理因素的改变有关,如夜间尿频、胃食管反流或肌肉骨骼不适,这些都是很重要的因素,很可能掩盖了激素的任何作用。内源性和外源性雌激素以及孕酮在围绝经期过渡期间与睡眠呈正相关。围绝经期激素治疗可显著改善睡眠障碍。由于在接受避孕治疗的年轻女性中未观察到这种效果,因此必须考虑睡眠障碍的其他原因,如衰老以及应激激素代谢的相关变化、血管舒缩症状的继发影响或抑郁。促性腺激素与睡眠障碍的关联小于卵巢激素,除了在围绝经期过渡期间,此时促卵泡激素与睡眠干扰有关。此外,多囊卵巢综合征女性中出现的高雄激素血症与睡眠障碍和特定的睡眠疾病有关,例如阻塞性睡眠呼吸暂停。