Zheng Sean L, Roddick Alistair J, Ayis Salma
1 Imperial College Healthcare NHS Trust, London, UK.
2 British Heart Foundation Centre of Research Excellence, Cardiovascular Division, King's College Hospital, London, UK.
Diab Vasc Dis Res. 2017 Sep;14(5):400-406. doi: 10.1177/1479164117715854. Epub 2017 Aug 27.
Aliskiren was shown to increase adverse events in patients with diabetes and concomitant renin-angiotensin blockade. We aim to investigate the efficacy and safety of aliskiren in patients with diabetes and increased cardiovascular risk or established cardiovascular disease.
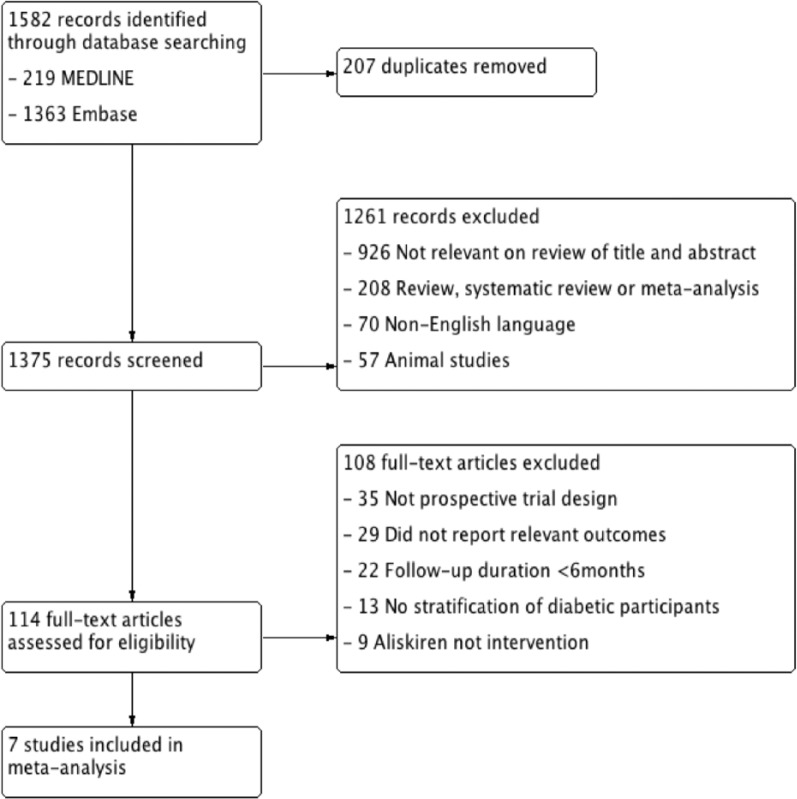
MEDLINE and Embase were searched for prospective studies comparing addition of aliskiren to standard medical therapy in patients with diabetes and cardiovascular disease, or ⩾1 additional cardiovascular risk factor (hypertension, abnormal lipid profile, microalbuminuria/proteinuria, chronic kidney disease). Relative risk for efficacy (all-cause mortality, combined cardiovascular mortality and hospitalisation) and safety (hyperkalaemia, hypotension, renal impairment) outcomes was calculated.
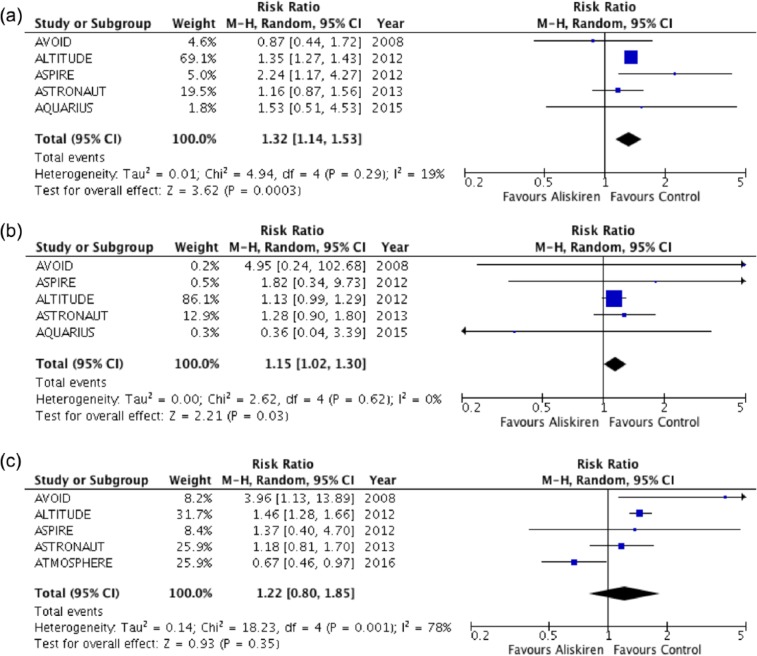
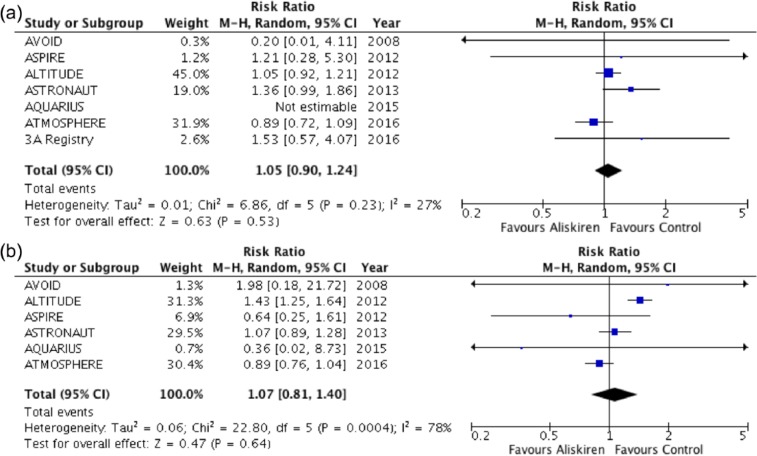
Of 2151 studies identified in the search, seven studies enrolling 13,395 patients were included. Aliskiren had no effect on all-cause mortality (relative risk: 1.05, 95% confidence interval: 0.90 to 1.24, p = 0.53), or combined cardiovascular mortality or heart failure hospitalisation (relative risk: 1.07, 95% confidence interval: 0.81 to 1.40, p = 0.64). Patients receiving aliskiren had a greater risk of developing hyperkalaemia (relative risk: 1.32, 95% confidence interval: 1.14 to 1.53, p = 0.0003) and renal impairment (relative risk: 1.15, 95% confidence interval: 1.02 to 1.30, p = 0.03), but not hypotension.
Patients with diabetes and cardiovascular disease or cardiovascular risk do not benefit from the addition of aliskiren to standard medical therapy. Detrimental safety profile in pooled analysis supports current warnings.
阿利吉仑已被证明会增加糖尿病患者以及同时使用肾素 - 血管紧张素阻滞剂患者的不良事件。我们旨在研究阿利吉仑在糖尿病患者且心血管风险增加或已确诊心血管疾病患者中的疗效和安全性。
在MEDLINE和Embase数据库中检索前瞻性研究,比较在糖尿病和心血管疾病患者或至少一种其他心血管风险因素(高血压、血脂异常、微量白蛋白尿/蛋白尿、慢性肾脏病)患者中,在标准药物治疗基础上加用阿利吉仑的情况。计算疗效(全因死亡率、心血管死亡率和住院率合并)和安全性(高钾血症、低血压、肾功能损害)结局的相对风险。
在检索到的2151项研究中,纳入了7项研究,共13395例患者。阿利吉仑对全因死亡率无影响(相对风险:1.05,95%置信区间:0.90至1.24,p = 0.53),对心血管死亡率和心力衰竭住院率合并情况也无影响(相对风险:1.07,95%置信区间:0.81至1.40,p = 0.64)。接受阿利吉仑治疗的患者发生高钾血症的风险更高(相对风险:1.32,95%置信区间:1.14至1.53,p = 0.0003)和肾功能损害的风险更高(相对风险:1.15,95%置信区间:1.02至1.30,p = 0.03),但对低血压无影响。
糖尿病和心血管疾病或心血管风险患者在标准药物治疗基础上加用阿利吉仑并无益处。汇总分析中不利的安全性情况支持当前的警告。