Yi Zinan, Mayorga Maria E, Orman Eric S, Wheeler Stephanie B, Hayashi Paul H, Barritt A Sidney
1 Operations Research Graduate Program, North Carolina State University, Raleigh, NC. 2 Department of Industrial and Systems Engineering, North Carolina State University, Raleigh, NC. 3 Department of Medicine, Indiana University School of Medicine, Indianapolis, IN. 4 Department of Health Policy and Management, University of North Carolina, Chapel Hill, NC. 5 Department of Medicine, University of North Carolina, Chapel Hill, NC.
Transplantation. 2017 Oct;101(10):2368-2374. doi: 10.1097/TP.0000000000001851.
Changes in the epidemiology of end-stage liver disease may lead to increased risk of dropout from the liver transplant waitlist. Anticipating the future of liver transplant waitlist characteristics is vital when considering organ allocation policy.
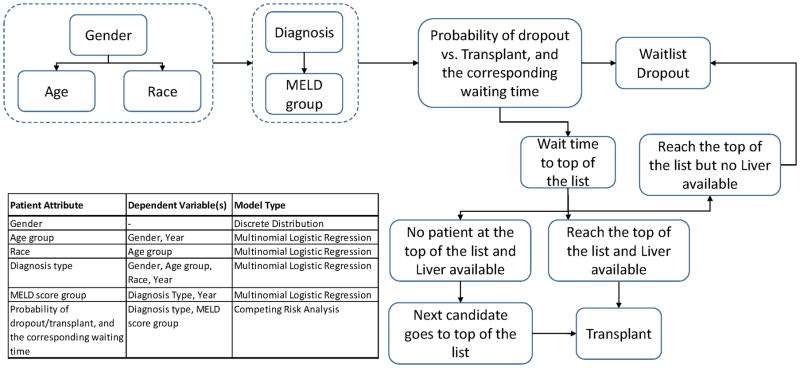
We performed a discrete event simulation to forecast patient characteristics and rate of waitlist dropout. Estimates were simulated from 2015 to 2025. The model was informed by data from the Organ Procurement and Transplant Network, 2003 to 2014. National data are estimated along with forecasts for 2 regions.
Nonalcoholic steatohepatitis will increase from 18% of waitlist additions to 22% by 2025. Hepatitis C will fall from 30% to 21%. Listings over age 60 years will increase from 36% to 48%. The hazard of dropout will increase from 41% to 46% nationally. Wait times for transplant for patients listed with a Model for End-Stage Liver Disease (MELD) between 22 and 27 will double. Region 5, which transplants at relatively higher MELD scores, will experience an increase from 53% to 64% waitlist dropout. Region 11, which transplants at lower MELD scores, will have an increase in waitlist dropout from 30% to 44%.
The liver transplant waitlist size will remain static over the next decade due to patient dropout. Liver transplant candidates will be older, more likely to have nonalcoholic steatohepatitis and will wait for transplantation longer even when listed at a competitive MELD score. There will continue to be significant heterogeneity among transplant regions where some patients will be more likely to drop out of the waitlist than receive a transplant.
终末期肝病流行病学的变化可能导致从肝移植等待名单上退出的风险增加。在考虑器官分配政策时,预测肝移植等待名单特征的未来情况至关重要。
我们进行了离散事件模拟,以预测患者特征和等待名单退出率。估计时间为2015年至2025年。该模型依据2003年至2014年器官获取与移植网络的数据构建。同时估计了全国数据以及两个地区的预测数据。
到2025年,非酒精性脂肪性肝炎在等待名单新增患者中的占比将从18%增至22%。丙型肝炎将从30%降至21%。60岁以上患者的登记比例将从36%增至48%。全国范围内退出等待名单的风险将从41%增至46%。终末期肝病模型(MELD)评分在22至27之间的患者的移植等待时间将翻倍。第5地区,其移植时的MELD评分相对较高,等待名单退出率将从53%增至64%。第11地区,其移植时的MELD评分较低,等待名单退出率将从30%增至44%。
由于患者退出,未来十年肝移植等待名单规模将保持稳定。肝移植候选者年龄将更大,更有可能患有非酒精性脂肪性肝炎,即使以有竞争力的MELD评分登记,等待移植的时间也会更长。移植地区之间仍将存在显著差异,一些患者从等待名单上退出的可能性高于接受移植的可能性。