Wiysonge Charles S, Ndze Valantine N, Kongnyuy Eugene J, Shey Muki S
Cochrane South Africa, South African Medical Research Council, Francie van Zijl Drive, Parow Valley, Cape Town, Western Cape, South Africa, 7505.
Cochrane Database Syst Rev. 2017 Sep 7;9(9):CD003648. doi: 10.1002/14651858.CD003648.pub4.
Strategies to reduce the risk of mother-to-child transmission of the human immunodeficiency virus (HIV) include lifelong antiretroviral therapy (ART) for HIV-positive women, exclusive breastfeeding from birth for six weeks plus nevirapine or replacement feeding plus nevirapine from birth for four to six weeks, elective Caesarean section delivery, and avoiding giving children chewed food. In some settings, these interventions may not be practical, feasible, or affordable. Simple, inexpensive, and effective interventions (that could potentially be implemented even in the absence of prenatal HIV testing programmes) would be valuable. Vitamin A, which plays a role in immune function, is one low-cost intervention that has been suggested in such settings.
To summarize the effects of giving vitamin A supplements to HIV-positive women during pregnancy and after delivery.
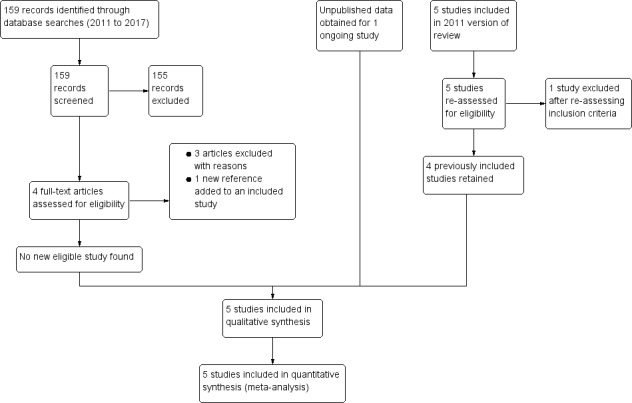
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Embase, and the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) up to 25 August 2017, and checked the reference lists of relevant articles for eligible studies.
We included randomized controlled trials conducted in any setting that compared vitamin A supplements to placebo or no intervention among HIV-positive women during pregnancy or after delivery, or both.
At least two review authors independently assessed study eligibility and extracted data. We expressed study results as risk ratios (RR) or mean differences (MD) as appropriate, with their 95% confidence intervals (CI), and conducted random-effects meta-analyses. This is an update of a review last published in 2011.
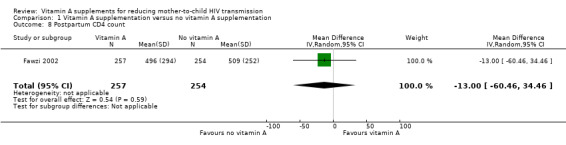
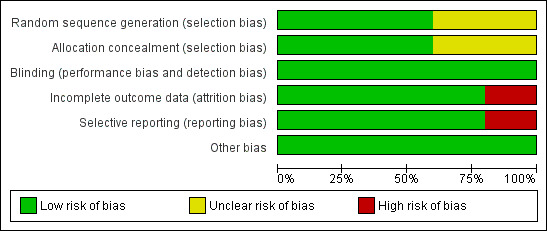
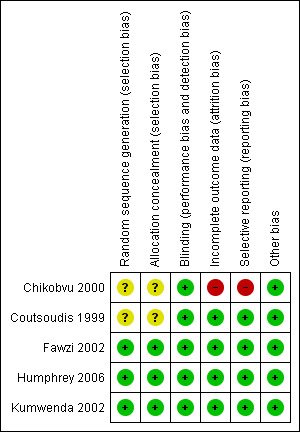
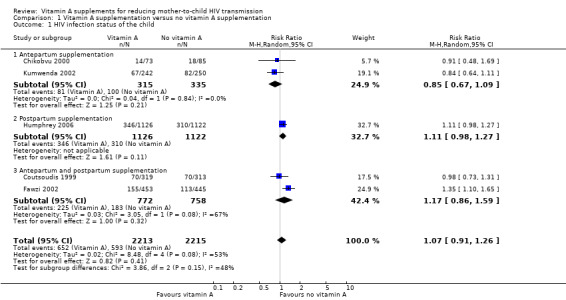
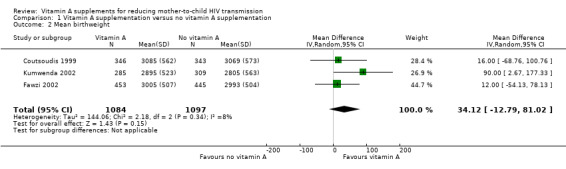
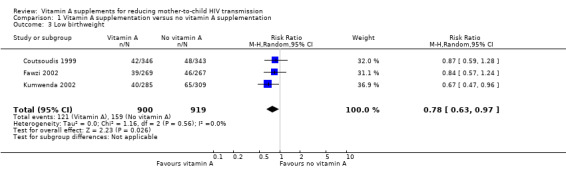
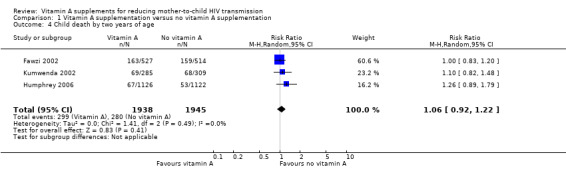
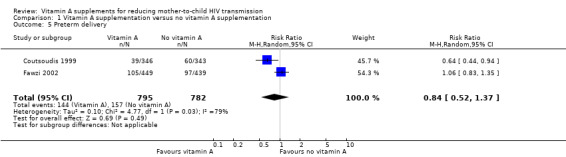
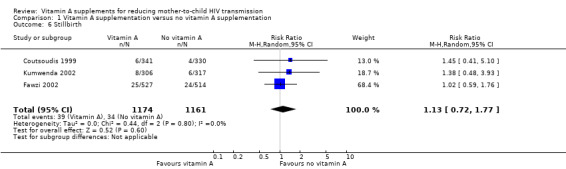
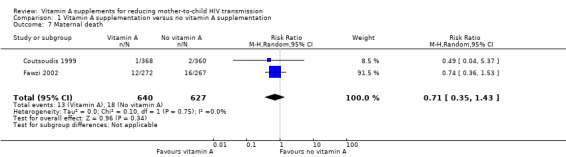
Five trials met the inclusion criteria. These were conducted in Malawi, South Africa, Tanzania, and Zimbabwe between 1995 and 2005 and none of the participants received ART. Women allocated to intervention arms received vitamin A supplements at a variety of doses (daily during pregnancy; a single dose immediately after delivery, or daily doses during pregnancy plus a single dose after delivery). Women allocated to comparison arms received identical placebo (6601 women, 4 trials) or no intervention (697 women, 1 trial). Four trials (with 6995 women) had low risk of bias and one trial (with 303 women) had high risk of attrition bias.The trials show that giving vitamin A supplements to HIV-positive women during pregnancy, the immediate postpartum period, or both, probably has little or no effect on mother-to-child transmission of HIV (RR 1.07, 95% CI 0.91 to 1.26; 4428 women, 5 trials, moderate certainty evidence) and may have little or no effect on child death by two years of age (RR 1.06, 95% CI 0.92 to 1.22; 3883 women, 3 trials, low certainty evidence). However, giving vitamin A supplements during pregnancy may increase the mean birthweight (MD 34.12 g, 95% CI -12.79 to 81.02; 2181 women, 3 trials, low certainty evidence) and probably reduces the incidence of low birthweight (RR 0.78, 95% CI 0.63 to 0.97; 1819 women, 3 trials, moderate certainty evidence); but we do not know whether vitamin A supplements affect the risk of preterm delivery (1577 women, 2 trials), stillbirth (2335 women, 3 trials), or maternal death (1267 women, 2 trials).
AUTHORS' CONCLUSIONS: Antepartum or postpartum vitamin A supplementation, or both, probably has little or no effect on mother-to-child transmission of HIV in women living with HIV infection and not on antiretroviral drugs. The intervention has largely been superseded by ART which is widely available and effective in preventing vertical transmission.
降低人类免疫缺陷病毒(HIV)母婴传播风险的策略包括对HIV阳性女性进行终身抗逆转录病毒治疗(ART)、从出生开始纯母乳喂养六周加奈韦拉平,或替代喂养加从出生开始使用奈韦拉平四至六周、选择性剖宫产以及避免给儿童喂食咀嚼过的食物。在某些情况下,这些干预措施可能不实用、不可行或难以负担。简单、廉价且有效的干预措施(即使在没有产前HIV检测项目的情况下也有可能实施)将很有价值。维生素A在免疫功能中发挥作用,是在此类情况下被建议采用的一种低成本干预措施。
总结孕期及产后给HIV阳性女性补充维生素A的效果。
我们检索了截至2017年8月25日的Cochrane对照试验中央登记库(CENTRAL)、PubMed、Embase以及世界卫生组织国际临床试验注册平台(WHO ICTRP),并检查了相关文章的参考文献列表以寻找符合条件的研究。
我们纳入了在任何环境中进行的随机对照试验,这些试验比较了孕期或产后或两者期间给HIV阳性女性补充维生素A与安慰剂或不进行干预的情况。
至少两名综述作者独立评估研究的合格性并提取数据。我们根据情况将研究结果表示为风险比(RR)或均值差(MD)及其95%置信区间(CI),并进行随机效应荟萃分析。这是对2011年发表的一篇综述的更新。
五项试验符合纳入标准。这些试验于1995年至2005年在马拉维、南非、坦桑尼亚和津巴布韦进行;没有参与者接受ART治疗。被分配到干预组的女性接受了各种剂量的维生素A补充剂(孕期每日服用;产后立即单次服用,或孕期每日服用加产后单次服用);被分配到对照组的女性接受相同的安慰剂(4项试验,6601名女性)或不进行干预(1项试验,697名女性)。四项试验(6995名女性)存在低偏倚风险,一项试验(303名女性)存在高失访偏倚风险;试验表明,孕期或产后或两者期间给HIV阳性女性补充维生素A可能对HIV母婴传播几乎没有影响(RR 1.07,95% CI 0.91至1.26;5项试验,4428名女性,中等确定性证据),并且可能对两岁儿童死亡几乎没有影响(RR 1.06, 95% CI 0.92至1.22;3项试验,3883名女性,低确定性证据)。然而,孕期补充维生素A可能会增加平均出生体重(MD 34.12 g,95% CI -12.79至81.02;3项试验,2181名女性,低确定性证据),并可能降低低出生体重的发生率(RR 0.78,95% CI 0.63至0.97;3项试验,1819名女性,中等确定性证据);但我们不知道维生素A补充剂是否会影响早产风险(2项试验,1577名女性)、死产风险(3项试验,2335名女性)或孕产妇死亡风险(2项试验,1267名女性)。
产前或产后补充维生素A,或两者同时补充,可能对感染HIV的女性的HIV母婴传播几乎没有影响,对接受抗逆转录病毒药物治疗的女性也没有影响。这种干预措施在很大程度上已被广泛可用且能有效预防垂直传播的ART所取代。