Siemieniuk Reed A, Foroutan Farid, Mirza Reza, Mah Ming Jinell, Alexander Paul E, Agarwal Arnav, Lesi Olufunmilayo, Merglen Arnaud, Chang Yaping, Zhang Yuan, Mir Hassan, Hepworth Elliot, Lee Yung, Zeraatkar Dena, Guyatt Gordon H
Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada.
Department of Medicine, University of Toronto, Toronto, Canada.
BMJ Open. 2017 Sep 11;7(9):e019022. doi: 10.1136/bmjopen-2017-019022.
To assess the impact of various antiretroviral/antiviral regimens in pregnant women living with HIV or hepatitis B virus (HBV).
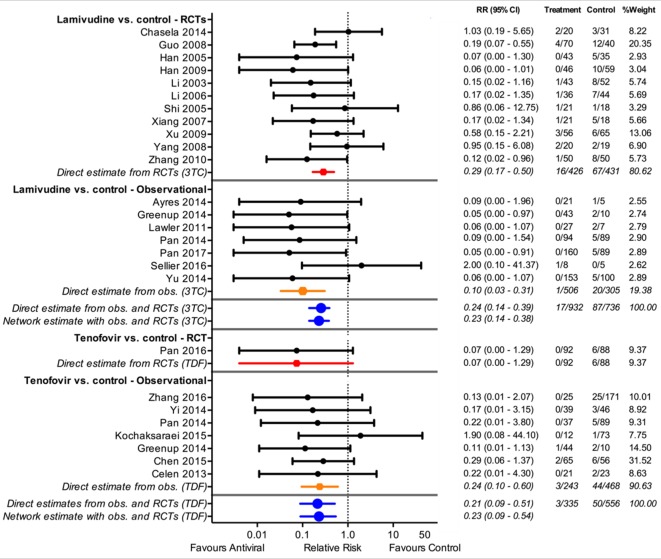
We performed random effects meta-analysis for HIV-related outcomes and network meta-analysis for HBV outcomes, and used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to assess quality separately for each outcome.
Embase and Medline to February 2017.
For maternal outcomes, we considered randomised controlled trials (RCTs) comparing tenofovir-based regimens with those with alternative nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs). For child outcomes, we included RCTs and comparative observational studies of tenofovir-based regimens versus alternative NRTIs regimens or, for HBV, placebo.
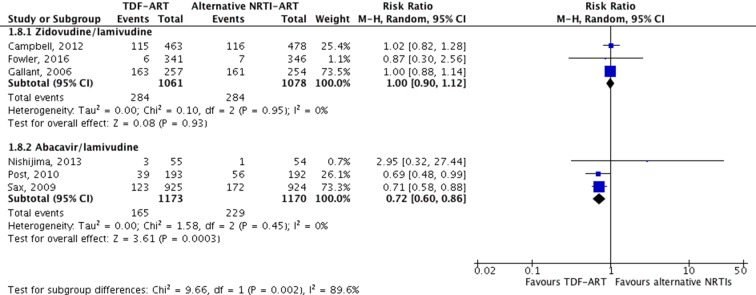
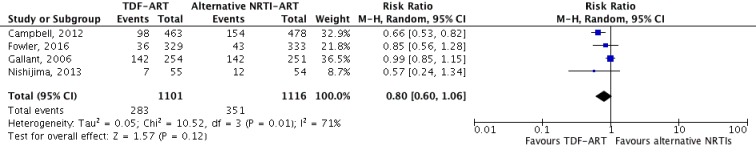
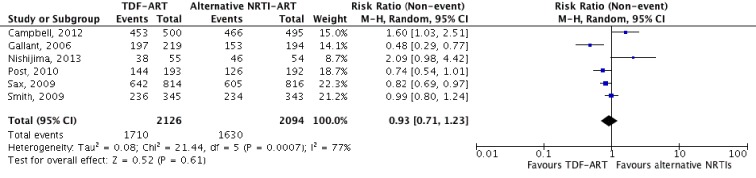
Ten studies (seven RCTs) met the inclusion criteria for maternal and child outcomes, and an additional 33 studies (12 RCTs) met the inclusion criteria for HBV-specific outcomes. The most common comparison was tenofovir and emtricitabine versus zidovudine and lamivudine. There was no apparent difference between tenofovir-based regimens and alternatives in maternal outcomes, including serious laboratory adverse events (low certainty) and serious clinical adverse events (moderate certainty). There was no difference between NRTIs in vertical transmission of HIV: 1 more per 1000, 8 fewer to 10 more, low certainty; or vertical transmission of HBV: 7 fewer per 1000, 10 fewer to 38 more, moderate certainty. We found moderate certainty evidence that tenofovir/emtricitabine increases the risk of stillbirths and early neonatal mortality (51 more per 1000, 11 more to 150 more) and the risk of early premature delivery at <34 weeks (42 more per 1000, 2 more to 127 more).
Tenofovir/emtricitabine is likely to increase stillbirth/early neonatal death and early premature delivery compared with zidovudine/lamivudine, but certainty is low when they are not coprescribed with lopinavir/ritonavir. Other outcomes are likely similar between antiretrovirals.
PROSPERO CRD42017054392.
评估各种抗逆转录病毒/抗病毒治疗方案对感染人类免疫缺陷病毒(HIV)或乙型肝炎病毒(HBV)的孕妇的影响。
我们对HIV相关结局进行随机效应荟萃分析,对HBV结局进行网状荟萃分析,并使用推荐分级评估、制定和评价(GRADE)框架对每个结局的质量进行单独评估。
截至2017年2月的Embase和Medline。
对于母亲结局,我们纳入了比较以替诺福韦为基础的治疗方案与使用其他核苷/核苷酸逆转录酶抑制剂(NRTIs)的随机对照试验(RCT)。对于儿童结局,我们纳入了以替诺福韦为基础的治疗方案与其他NRTIs治疗方案或(对于HBV)安慰剂的RCT和比较观察性研究。
10项研究(7项RCT)符合母亲和儿童结局的纳入标准,另外33项研究(12项RCT)符合HBV特异性结局的纳入标准。最常见的比较是替诺福韦和恩曲他滨与齐多夫定和拉米夫定。在母亲结局方面,包括严重实验室不良事件(确定性低)和严重临床不良事件(确定性中等),以替诺福韦为基础的治疗方案与其他方案之间没有明显差异。在HIV垂直传播方面,NRTIs之间没有差异:每1000例中多1例,少8例至多10例,确定性低;或在HBV垂直传播方面:每1000例中少7例,少10例至多38例,确定性中等。我们发现有中等确定性证据表明,替诺福韦/恩曲他滨会增加死产和早期新生儿死亡的风险(每1000例中多51例,多11例至多150例)以及<34周早产的风险(每1000例中多42例,多2例至多127例)。
与齐多夫定/拉米夫定相比,替诺福韦/恩曲他滨可能会增加死产/早期新生儿死亡和早产的风险,但当它们未与洛匹那韦/利托那韦联合使用时,确定性较低。抗逆转录病毒药物在其他结局方面可能相似。
PROSPERO CRD42017054392。