Department of Radiation Oncology, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania.
Department of Radiation Oncology, Cleveland Clinic, Cleveland, Ohio.
Int J Radiat Oncol Biol Phys. 2018 Mar 1;100(3):595-605. doi: 10.1016/j.ijrobp.2017.04.017. Epub 2017 Apr 24.
Two modern methods of reirradiation, intensity modulated radiation therapy (IMRT) and stereotactic body radiation therapy (SBRT), are established for patients with recurrent or second primary squamous cell carcinoma of the head and neck (rSCCHN). We performed a retrospective multi-institutional analysis to compare methods.
Data from patients with unresectable rSCCHN previously irradiated to ≥40 Gy who underwent reirradiation with IMRT or SBRT were collected from 8 institutions. First, the prognostic value of our IMRT-based recursive partitioning analysis (RPA) separating those patients with unresectable tumors with an intertreatment interval >2 years or those with ≤2 years and without feeding tube or tracheostomy dependence (class II) from other patients with unresected tumors (class III) was investigated among SBRT patients. Overall survival (OS) and locoregional failure were then compared between IMRT and SBRT by use of 2 methods to control for baseline differences: Cox regression weighted by the inverse probability of treatment and subset analysis by RPA classification.
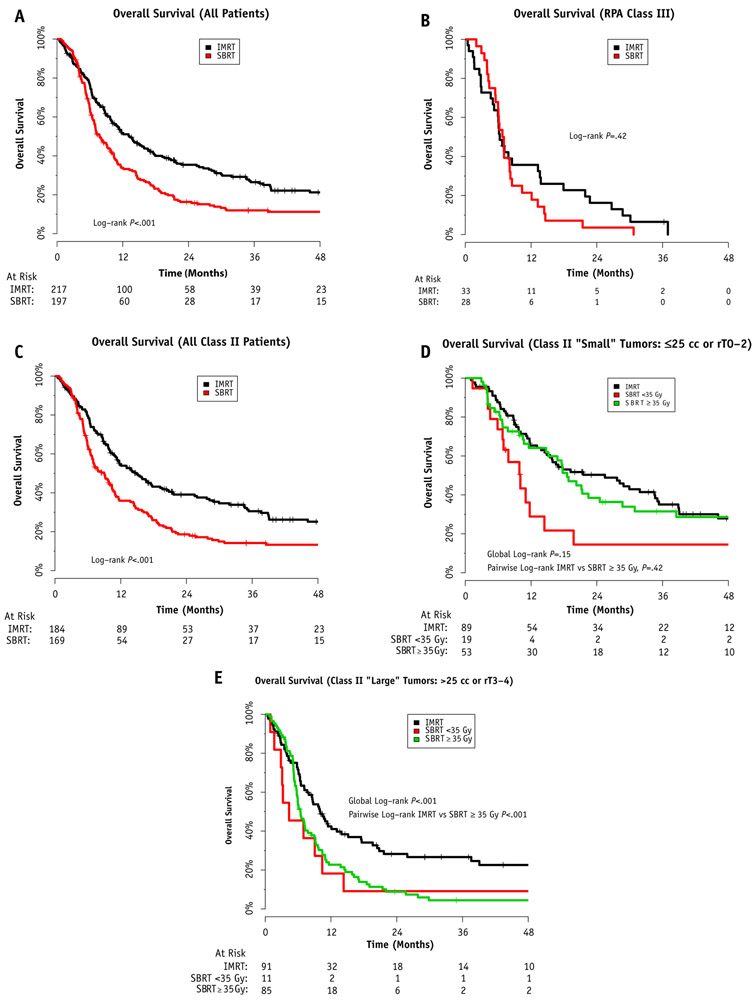
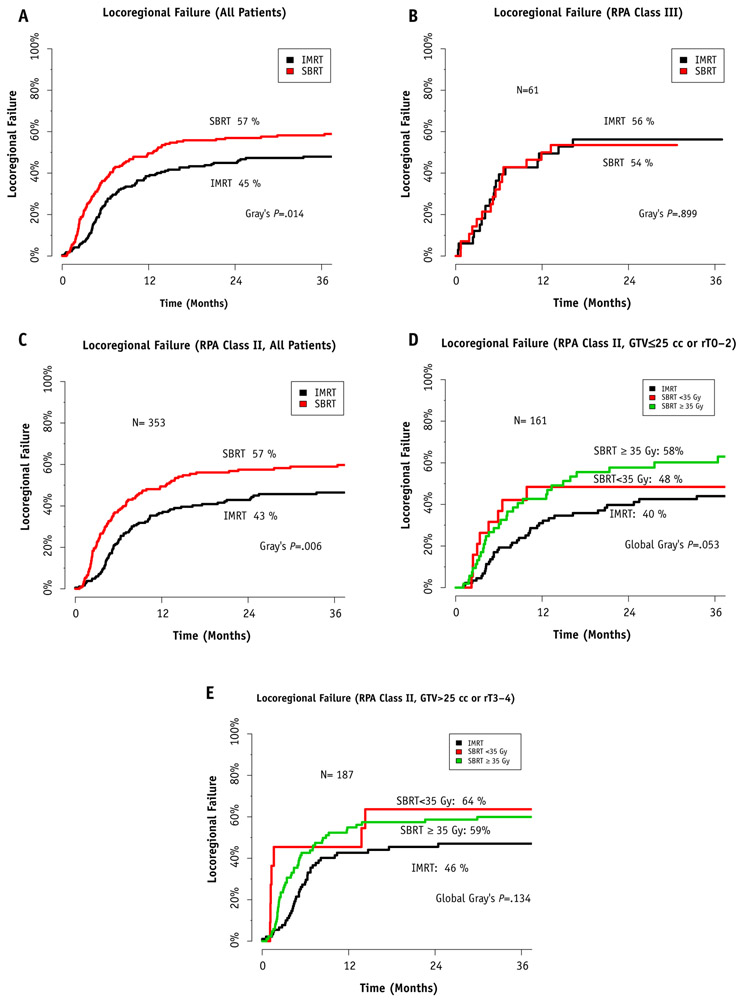
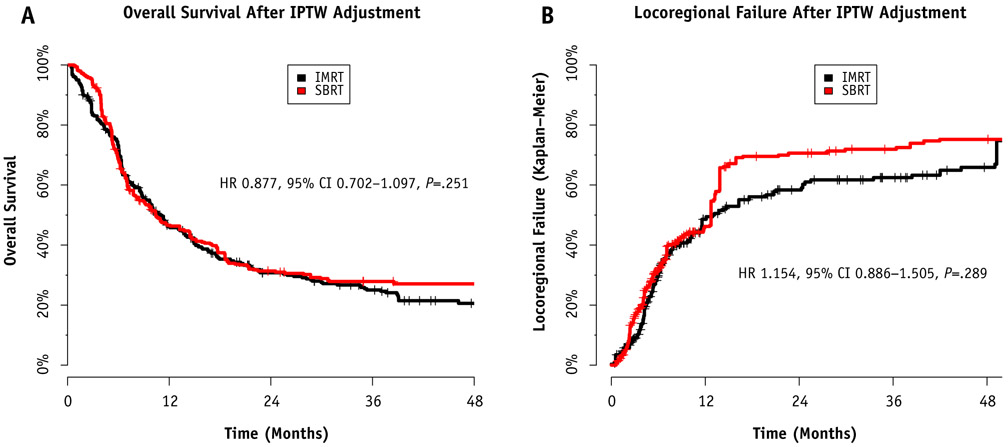
The study included 414 patients with unresectable rSCCHN: 217 with IMRT and 197 with SBRT. The unadjusted 2-year OS rate was 35.4% for IMRT and 16.3% for SBRT (P<.01). Among SBRT patients, RPA classification retained an independent association with OS. On Cox regression weighted by the inverse probability of treatment, no significant differences in OS or locoregional failure between IMRT and SBRT were demonstrated. Analysis by RPA class showed similar OS between IMRT and SBRT for class III patients. In all class II patients, IMRT was associated with improved OS (P<.001). Further subset analysis demonstrated comparable OS when ≥35 Gy was delivered with SBRT to small tumor volumes. Acute grade ≥4 toxicity was greater in the IMRT group than in the SBRT group (5.1% vs 0.5%, P<.01), with no significant difference in late toxicity.
Reirradiation both with SBRT and with IMRT appear relatively safe with favorable toxicity compared with historical studies. Outcomes vary by RPA class, which informs clinical trial design. Survival is poor in class III patients, and alternative strategies are needed.
调强放疗(IMRT)和立体定向体部放疗(SBRT)是两种用于治疗复发性或第二原发头颈部鳞状细胞癌(rSCCHN)的现代再放疗方法。我们进行了一项回顾性多机构分析,以比较这两种方法。
从 8 个机构收集了先前接受过≥40Gy 放疗且无法切除的 rSCCHN 患者,这些患者接受了 IMRT 或 SBRT 再放疗。首先,在 SBRT 患者中,我们研究了基于我们的调强放疗递归分区分析(RPA)的预后价值,该分析将那些有治疗间隔>2 年或≤2 年且无喂养管或气管造口术依赖(II 级)的无法切除肿瘤的患者与其他无法切除肿瘤(III 级)的患者分开。然后,通过使用 2 种方法来控制基线差异,即通过治疗逆概率加权的 Cox 回归和 RPA 分类的亚组分析,比较了 IMRT 和 SBRT 之间的总生存(OS)和局部区域失败。
本研究包括 414 例无法切除的 rSCCHN 患者:217 例接受 IMRT,197 例接受 SBRT。未调整的 2 年 OS 率分别为 IMRT 组的 35.4%和 SBRT 组的 16.3%(P<.01)。在 SBRT 患者中,RPA 分类仍然与 OS 独立相关。通过治疗逆概率加权的 Cox 回归,IMRT 和 SBRT 之间的 OS 或局部区域失败无显著差异。通过 RPA 分类分析,对于 III 级患者,IMRT 和 SBRT 的 OS 相似。在所有 II 级患者中,IMRT 与 OS 改善相关(P<.001)。进一步的亚组分析表明,当 SBRT 给予≥35Gy 时,对于小肿瘤体积,OS 可与 SBRT 相媲美。IMRT 组的急性 3 级以上毒性发生率高于 SBRT 组(5.1%比 0.5%,P<.01),但晚期毒性无显著差异。
与历史研究相比,SBRT 和 IMRT 再放疗都相对安全,毒性良好。结果因 RPA 分类而异,这为临床试验设计提供了信息。III 级患者的生存较差,需要有其他的治疗策略。