Pattison Sharon, Mitchell Catherine, Lade Stephen, Leong Trevor, Busuttil Rita A, Boussioutas Alex
Department of Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand.
Department of Pathology, Peter MacCallum Cancer Centre, Parkville, Victoria, Australia.
PLoS One. 2017 Sep 18;12(9):e0183891. doi: 10.1371/journal.pone.0183891. eCollection 2017.
Survival from gastric cancer remains poor, particularly in Western populations. Previous pre-clinical and subgroup analyses of clinical trials have suggested differing benefits from fluoropyrimidine-based chemotherapeutics for diffuse and intestinal gastric cancer. This analysis examines patterns of relapse with and without adjuvant chemotherapy after curative resection for gastric cancer in these subtypes to explore the Lauren classification as a predictive marker of benefit for fluoropyrimidine-based adjuvant chemotherapy.
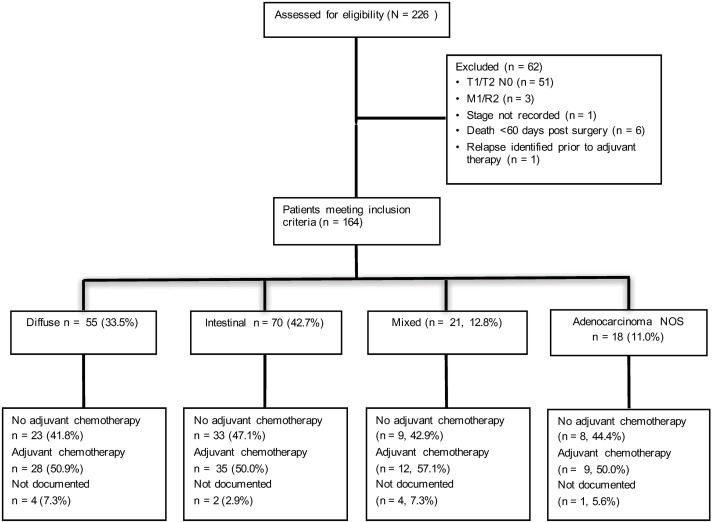
Gastric cancer patients enrolled in an ongoing tissue banking study were analysed, 164 patients who would currently be considered for adjuvant therapy after curative resection were included in the analysis. Patients who did and did not receive adjuvant chemotherapy were compared. The primary end point was relapse free survival.
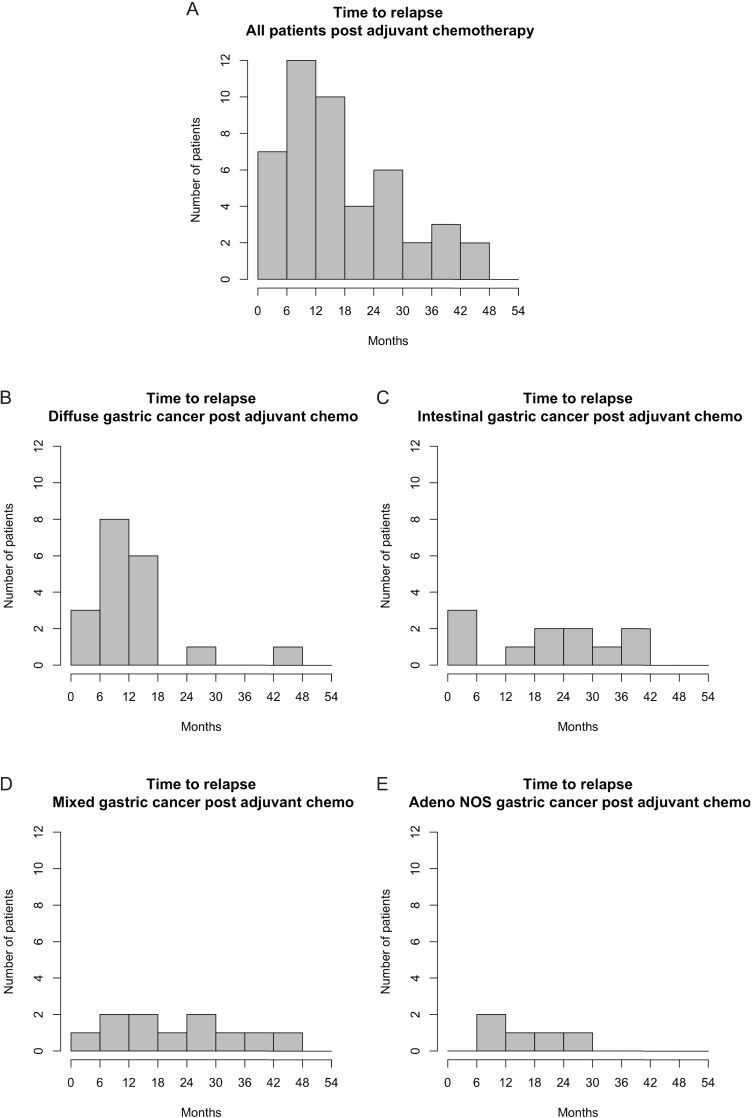
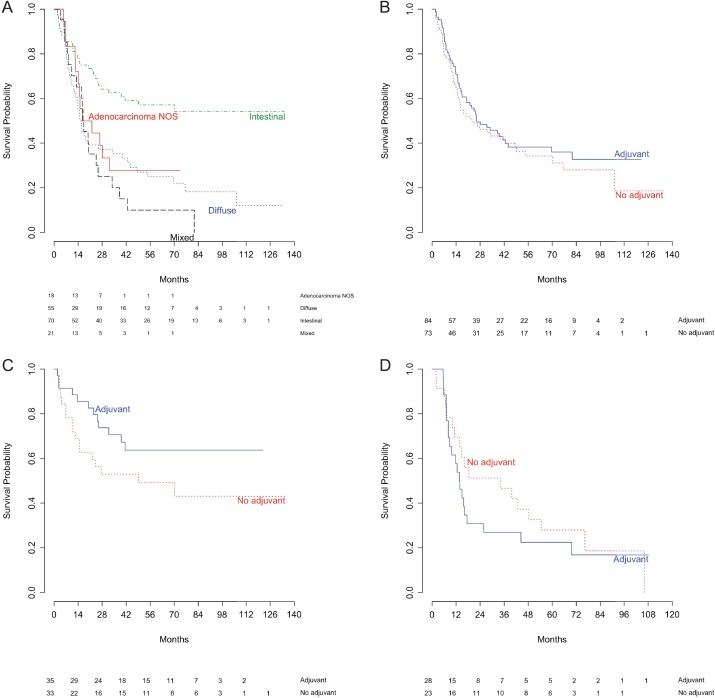
Approximately 50% of patients received adjuvant chemotherapy, the majority receiving a fluoropyrimidine-based regimen. The comparison of Kaplan-Meier curves for patients who did and did not receive adjuvant chemotherapy are different between patients with intestinal and diffuse gastric cancer, and suggest that there may be a benefit in intestinal gastric cancer. The hazard ratio for adjuvant chemotherapy for intestinal gastric cancer was 0.56, (95% CI 0.27-1.17), suggesting a trend towards benefit that was lacking in diffuse gastric cancer patients (1.26, 95% CI 0.70-2.38). The patterns of relapse after adjuvant chemotherapy also differed between diffuse and intestinal gastric cancer. More than 50% of diffuse gastric cancer patients who received adjuvant chemotherapy relapsed within 12 months of surgery despite similar surgical parameters.
Lauren classification is prognostic in gastric cancer. This analysis adds further evidence that it may also be predictive of benefit for fluoropyrimidine-based chemotherapeutics, with lower chemosensitivity seen in diffuse gastric cancer. Treating diffuse and intestinal gastric cancer as separate entities, with identification of efficacious treatments for diffuse gastric cancer will help in improving outcomes from gastric cancer.
胃癌患者的生存率仍然很低,尤其是在西方人群中。先前的临床前研究和临床试验亚组分析表明,基于氟嘧啶的化疗药物对弥漫型和肠型胃癌有不同的疗效。本分析研究了这些亚型的胃癌患者在根治性切除术后接受和未接受辅助化疗的复发模式,以探讨劳伦分类法作为基于氟嘧啶的辅助化疗获益预测指标的可能性。
对参与一项正在进行的组织库研究的胃癌患者进行分析,分析纳入了164例目前被认为可在根治性切除术后接受辅助治疗的患者。比较了接受和未接受辅助化疗的患者。主要终点是无复发生存期。
约50%的患者接受了辅助化疗,大多数接受基于氟嘧啶的方案。接受和未接受辅助化疗患者的Kaplan-Meier曲线比较在肠型和弥漫型胃癌患者中有所不同,提示肠型胃癌可能获益。肠型胃癌辅助化疗的风险比为0.56(95%CI 0.27-1.17),提示有获益趋势,而弥漫型胃癌患者则无此趋势(1.26,95%CI 0.70-2.38)。辅助化疗后的复发模式在弥漫型和肠型胃癌之间也有所不同。尽管手术参数相似,但超过50%接受辅助化疗的弥漫型胃癌患者在术后12个月内复发。
劳伦分类法对胃癌具有预后价值。本分析进一步证明,它也可能预测基于氟嘧啶的化疗药物的获益情况,弥漫型胃癌的化疗敏感性较低。将弥漫型和肠型胃癌视为不同实体,确定弥漫型胃癌的有效治疗方法将有助于改善胃癌的治疗效果。