Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Republic of Korea.
Department of Surgery, Yonsei University College of Medicine, Seoul, Republic of Korea.
Int J Med Sci. 2017 Aug 18;14(10):951-960. doi: 10.7150/ijms.20347. eCollection 2017.
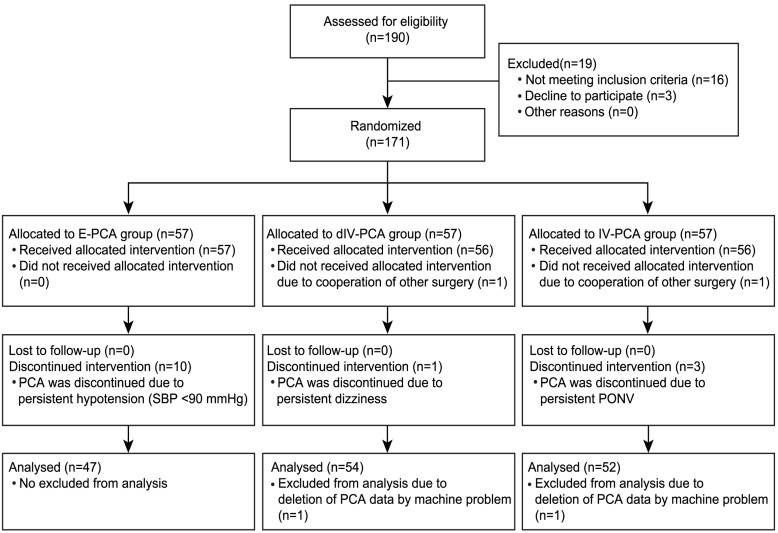
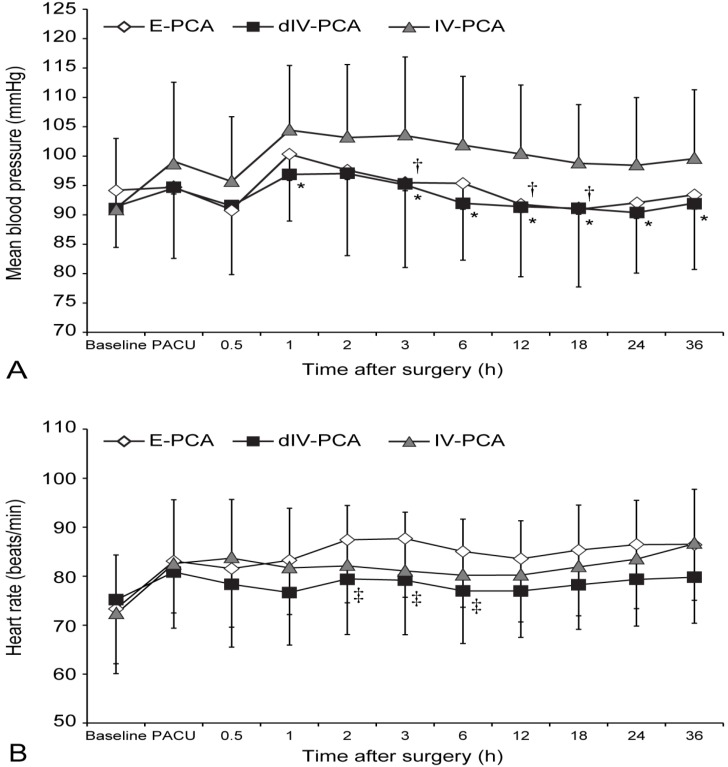
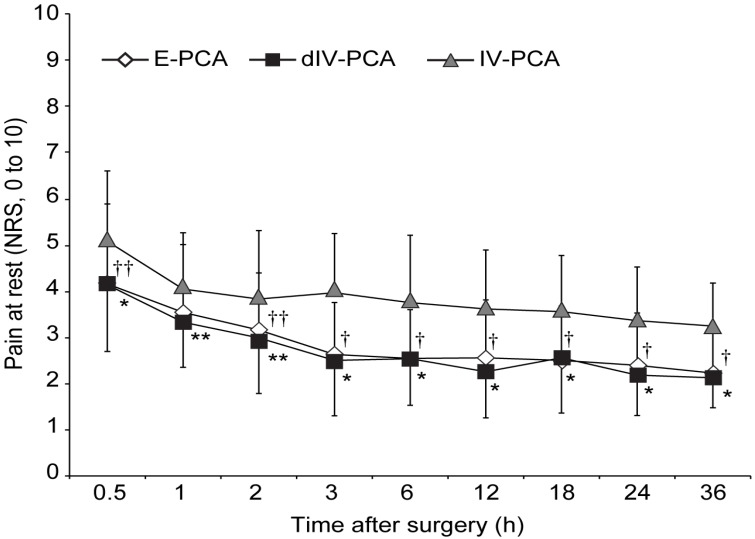
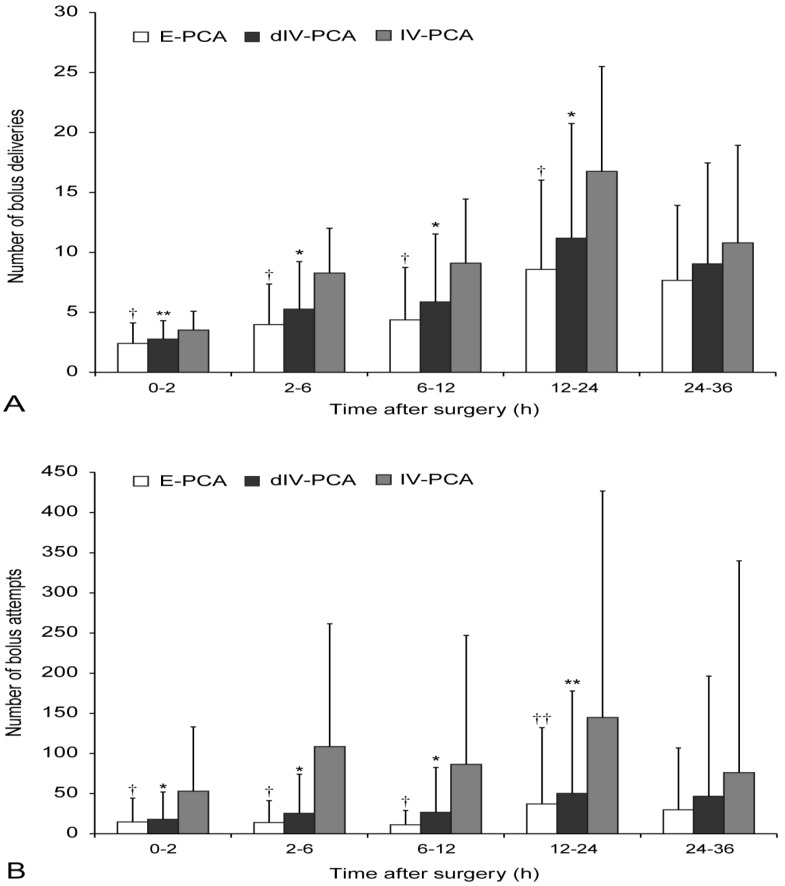
This study was investigated the effects of dexmedetomidine in combination with fentanyl-based intravenous patient-controlled analgesia (IV-PCA) on pain attenuation in patients undergoing open gastrectomy in comparison with conventional thoracic epidural patient-controlled analgesia (E-PCA) and IV-PCA. : One hundred seventy-one patients who planned open gastrectomy were randomly distributed into one of the 3 groups: conventional thoracic E-PCA (E-PCA group, n = 57), dexmedetomidine in combination with fentanyl-based IV-PCA (dIV-PCA group, n = 57), or fentanyl-based IV-PCA only (IV-PCA group, n = 57). The primary outcome was the postoperative pain intensity (numerical rating scale) at 3 hours after surgery, and the secondary outcomes were the number of bolus deliveries and bolus attempts, and the number of patients who required additional rescue analgesics. Mean blood pressure, heart rate, and adverse effects were evaluated as well. One hundred fifty-three patients were finally completed the study. The postoperative pain intensity was significantly lower in the dIV-PCA and E-PCA groups than in the IV-PCA group, but comparable between the dIV-PCA group and the E-PCA group. Patients in the dIV-PCA and E-PCA groups needed significantly fewer additional analgesic rescues between 6 and 24 hours after surgery, and had a significantly lower number of bolus attempts and bolus deliveries during the first 24 hours after surgery than those in the IV-PCA group. Dexmedetomidine in combination with fentanyl-based IV-PCA significantly improved postoperative analgesia in patients undergoing open gastrectomy without hemodynamic instability, which was comparable to thoracic E-PCA. Furthermore, this approach could be clinically more meaningful owing to its noninvasive nature.
这项研究旨在比较右美托咪定联合芬太尼静脉患者自控镇痛(IV-PCA)与传统胸椎硬膜外患者自控镇痛(E-PCA)和 IV-PCA 在减轻开腹胃切除术后疼痛方面的效果。将计划接受开腹胃切除术的 171 名患者随机分为三组:常规胸椎 E-PCA(E-PCA 组,n = 57)、右美托咪定联合芬太尼 IV-PCA(dIV-PCA 组,n = 57)或芬太尼 IV-PCA 仅(IV-PCA 组,n = 57)。主要结局是术后 3 小时的疼痛强度(数字评分量表),次要结局是推注次数和推注尝试次数,以及需要额外解救性镇痛的患者人数。还评估了平均血压、心率和不良反应。最后,153 名患者完成了研究。dIV-PCA 和 E-PCA 组的术后疼痛强度明显低于 IV-PCA 组,但 dIV-PCA 组与 E-PCA 组之间无差异。dIV-PCA 和 E-PCA 组在术后 6 至 24 小时内需要的额外镇痛解救明显较少,且在术后 24 小时内的推注尝试和推注次数明显少于 IV-PCA 组。右美托咪定联合芬太尼 IV-PCA 可显著改善开腹胃切除术患者的术后镇痛效果,且不引起血流动力学不稳定,与胸椎 E-PCA 相当。此外,由于其非侵入性,这种方法在临床上可能更有意义。