Sadeghirad Behnam, Siemieniuk Reed A C, Brignardello-Petersen Romina, Papola Davide, Lytvyn Lyubov, Vandvik Per Olav, Merglen Arnaud, Guyatt Gordon H, Agoritsas Thomas
Department of Health Research Methods, Evidence, and Impact (HEI), McMaster University, Hamilton, ON, Canada
HIV/STI Surveillance Research Centre, and WHO Collaborating Centre for HIV Surveillance, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran.
BMJ. 2017 Sep 20;358:j3887. doi: 10.1136/bmj.j3887.
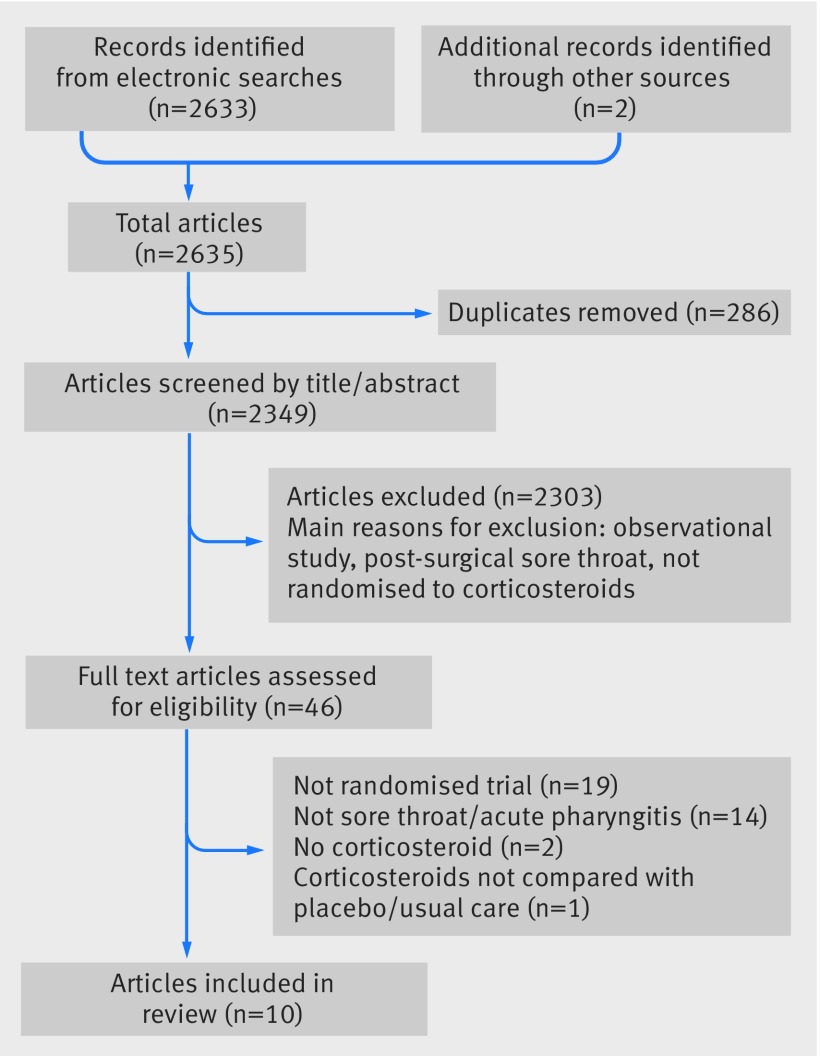
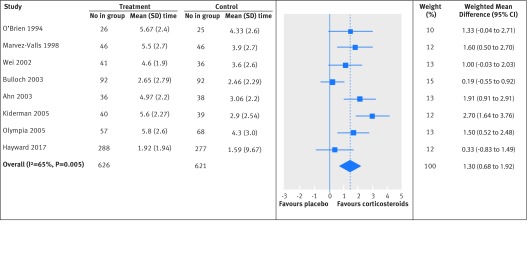
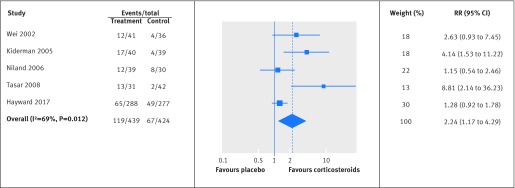
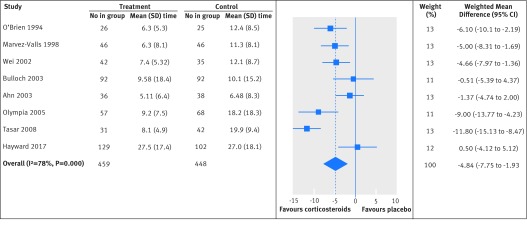
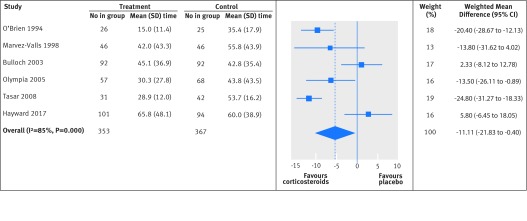
To estimate the benefits and harms of using corticosteroids as an adjunct treatment for sore throat. Systematic review and meta-analysis of randomised control trials. Medline, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), trial registries up to May 2017, reference lists of eligible trials, related reviews. Randomised controlled trials of the addition of corticosteroids to standard clinical care for patients aged 5 or older in emergency department and primary care settings with clinical signs of acute tonsillitis, pharyngitis, or the clinical syndrome of sore throat. Trials were included irrespective of language or publication status. Reviewers identified studies, extracted data, and assessed the quality of the evidence, independently and in duplicate. A parallel guideline committee ( Rapid Recommendation) provided input on the design and interpretation of the systematic review, including the selection of outcomes important to patients. Random effects model was used for meta-analyses. Quality of evidence was assessed with the GRADE approach. 10 eligible trials enrolled 1426 individuals. Patients who received single low dose corticosteroids (the most common intervention was oral dexamethasone with a maximum dose of 10 mg) were twice as likely to experience pain relief after 24 hours (relative risk 2.2, 95% confidence interval 1.2 to 4.3; risk difference 12.4%; moderate quality evidence) and 1.5 times more likely to have no pain at 48 hours (1.5, 1.3 to 1.8; risk difference 18.3%; high quality). The mean time to onset of pain relief in patients treated with corticosteroids was 4.8 hours earlier (95% confidence interval -1.9 to -7.8; moderate quality) and the mean time to complete resolution of pain was 11.1 hours earlier (-0.4 to -21.8; low quality) than in those treated with placebo. The absolute pain reduction at 24 hours (visual analogue scale 0-10) was greater in patients treated with corticosteroids (mean difference 1.3, 95% confidence interval 0.7 to 1.9; moderate quality). Nine of the 10 trials sought information regarding adverse events. Six studies reported no adverse effects, and three studies reported few adverse events, which were mostly complications related to disease, with a similar incidence in both groups. Single low dose corticosteroids can provide pain relief in patients with sore throat, with no increase in serious adverse effects. Included trials did not assess the potential risks of larger cumulative doses in patients with recurrent episodes of acute sore throat. PROSPERO CRD42017067808.
评估使用皮质类固醇作为咽喉痛辅助治疗的益处和危害。对随机对照试验进行系统评价和荟萃分析。检索了截至2017年5月的Medline、Embase、Cochrane对照试验中央注册库(CENTRAL)、试验注册库、符合条件试验的参考文献列表以及相关综述。纳入急诊科和初级保健机构中5岁及以上有急性扁桃体炎、咽炎或咽喉痛临床综合征体征的患者,在标准临床护理基础上加用皮质类固醇的随机对照试验。试验纳入不考虑语言或发表状态。综述作者独立且重复地识别研究、提取数据并评估证据质量。一个平行的指南委员会(快速推荐)为系统评价的设计和解释提供了意见,包括选择对患者重要的结局指标。采用随机效应模型进行荟萃分析。使用GRADE方法评估证据质量。10项符合条件的试验纳入了1426名个体。接受单次低剂量皮质类固醇治疗(最常见的干预措施是口服地塞米松,最大剂量为10毫克)的患者在24小时后疼痛缓解的可能性是未接受治疗患者的两倍(相对危险度2.2,95%置信区间1.2至4.3;风险差值12.4%;中等质量证据),在48小时时无疼痛的可能性高出1.5倍(1.5,1.3至1.8;风险差值18.3%;高质量)。与接受安慰剂治疗的患者相比,接受皮质类固醇治疗的患者疼痛缓解开始的平均时间提前4.8小时(95%置信区间-1.9至-7.8;中等质量),疼痛完全缓解的平均时间提前11.1小时(-0.4至-21.8;低质量)。在24小时时(视觉模拟评分0-10),接受皮质类固醇治疗的患者绝对疼痛减轻程度更大(平均差值1.3,95%置信区间0.7至1.9;中等质量)。10项试验中的9项收集了不良事件信息。6项研究报告无不良反应,3项研究报告不良事件较少,且大多为与疾病相关的并发症,两组发生率相似。单次低剂量皮质类固醇可为咽喉痛患者缓解疼痛,且不会增加严重不良反应。纳入的试验未评估急性咽喉痛反复发作患者使用更大累积剂量的潜在风险。国际前瞻性系统评价注册库(PROSPERO)注册号:CRD42017067808 。