Tan Aaron C, Li Bob T, Nahar Kazi, Danieletto Suzanne, Fong Eva S, Currer Trevor, Parasyn Andrew, Middleton Philip, Wong Heidi, Smart Denis, Rutovitz Josie J, McCloud Philip, Hughes T Michael, Marx Gavin M
SAN Integrated Cancer Centre, Sydney Adventist Hospital, Wahroonga, Australia.
Division of Solid Tumor Oncology, Department of Medicine, Memorial Sloan Kettering Cancer Center, and Weill Cornell Medical College, New York, NY, USA.
Asia Pac J Clin Oncol. 2018 Apr;14(2):e161-e166. doi: 10.1111/ajco.12779. Epub 2017 Sep 29.
Decisions regarding adjuvant chemotherapy for early breast cancer are complex. Ki67 is increasingly used, in conjunction with conventional prognostic markers, to help decide the use of adjuvant chemotherapy for early breast cancer. Ki67 has been proposed as an economical alternative to Oncotype DX recurrence score (RS), which is a validated prognostic marker for disease recurrence and predictive marker for benefit from chemotherapy. This study aimed to determine in patients where conventional prognostic markers did not provide a clear recommendation for adjuvant chemotherapy, whether Ki67 could be a substitute for RS.
We reviewed all cases of luminal-type node-negative early breast cancer (T1-2, N0-1mi, M0, estrogen receptor positive, HER2 negative) referred for Oncotype DX testing by the multidisciplinary team at an Australian tertiary private hospital from 14th December 2006 to 31st December 2013, when conventional prognostic markers did not provide a clear recommendation for adjuvant chemotherapy. RS was correlated with Ki67, along with other conventional prognostic markers including tumor size, grade, mitotic rate and lymphovascular invasion. Spearman's rank order correlation coefficient and Pearson product-moment correlation coefficient (r) were used for ordinal and continuous variables, respectively.
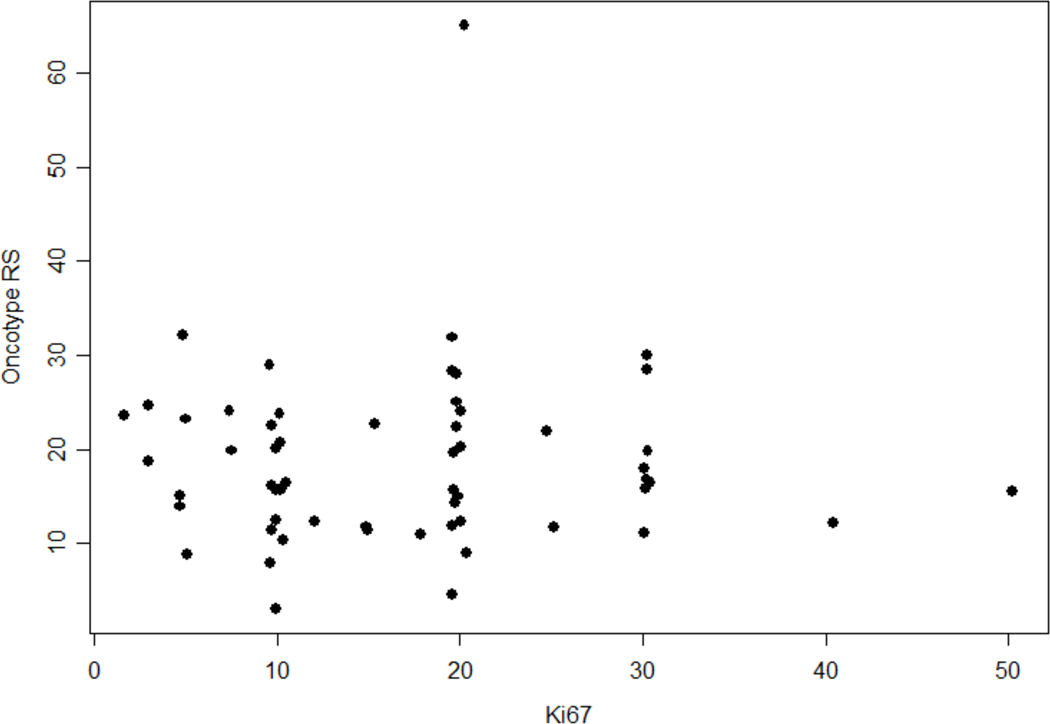
A total of 58 patients were analyzed, median Ki67 was 15% (range 2-50%) and the median RS was 16 (range 3-65). There was no positive correlation between Ki67 and RS (r = 0.01, P = 0.93). No single conventional prognostic marker was shown to significantly correlate with RS, including tumor size (r = -0.02, P = 0.88), grade (r = 0.10, P = 0.44), mitotic rate (r = -0.07, P = 0.69) and lymphovascular invasion (r = -0.12, P = 0.39).
Ki67 and conventional prognostic markers do not correlate with Oncotype DX RS. In the setting where conventional prognostic markers do not show a clear indication for or against adjuvant chemotherapy as determined by consensus in a multidisciplinary team, Ki67 is not a substitute for Oncotype DX testing. RS may provide additional information to aid decision making for adjuvant chemotherapy.
早期乳腺癌辅助化疗的决策复杂。Ki67越来越多地与传统预后标志物一起用于辅助决策早期乳腺癌辅助化疗的使用。Ki67已被提议作为Oncotype DX复发评分(RS)的经济替代指标,RS是疾病复发的有效预后标志物和化疗获益的预测标志物。本研究旨在确定在传统预后标志物未对辅助化疗提供明确建议的患者中,Ki67是否可替代RS。
我们回顾了2006年12月14日至2013年12月31日期间,澳大利亚一家三级私立医院多学科团队转诊进行Oncotype DX检测的所有腔面型淋巴结阴性早期乳腺癌(T1-2,N0-1mi,M0,雌激素受体阳性,HER2阴性)病例,此时传统预后标志物未对辅助化疗提供明确建议。将RS与Ki67以及其他传统预后标志物(包括肿瘤大小、分级、有丝分裂率和淋巴管浸润)进行相关性分析。Spearman等级相关系数和Pearson积矩相关系数(r)分别用于有序变量和连续变量。
共分析了58例患者,Ki67中位数为15%(范围2-50%),RS中位数为16(范围3-65)。Ki67与RS之间无正相关(r = 0.01,P = 0.93)。未显示单一传统预后标志物与RS显著相关,包括肿瘤大小(r = -0.02,P = 0.88)、分级(r = 0.10,P = 0.44)、有丝分裂率(r = -0.07,P = 0.69)和淋巴管浸润(r = -0.12,P = 0.39)。
Ki67和传统预后标志物与Oncotype DX RS不相关。在多学科团队共识确定传统预后标志物未明确显示辅助化疗的支持或反对指征的情况下,Ki67不能替代Oncotype DX检测。RS可能提供额外信息以辅助辅助化疗的决策。