Lehmann Clara, Kochanek Matthias, Abdulla Diana, Becker Stephan, Böll Boris, Bunte Anne, Cadar Daniel, Dormann Arno, Eickmann Markus, Emmerich Petra, Feldt Torsten, Frank Christina, Fries Jochen, Gabriel Martin, Goetsch Udo, Gottschalk René, Günther Stephan, Hallek Michael, Häussinger Dieter, Herzog Christian, Jensen Björn, Kolibay Felix, Krakau Michael, Langebartels Georg, Rieger Toni, Schaade Lars, Schmidt-Chanasit Jonas, Schömig Edgar, Schüttfort Gundolf, Shimabukuro-Vornhagen Alexander, von Bergwelt-Baildon Michael, Wieland Ulrike, Wiesmüller Gerhard, Wolf Timo, Fätkenheuer Gerd
Department I of Internal Medicine, University of Cologne, Germany.
German Center for Infection Research (DZIF), Bonn-Cologne, Germany.
Euro Surveill. 2017 Sep;22(39). doi: 10.2807/1560-7917.ES.2017.22.39.17-00088.
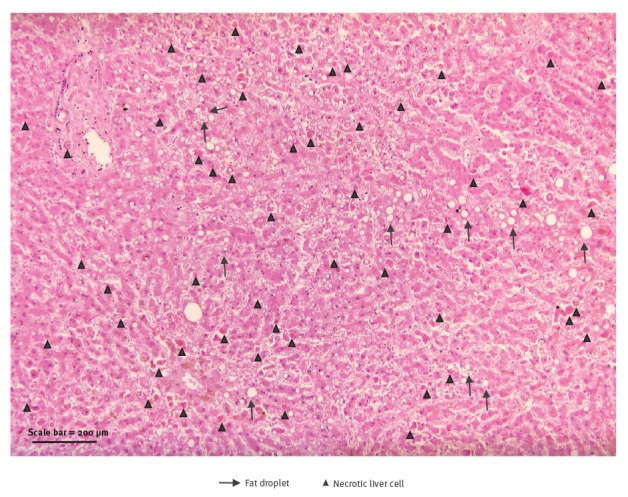
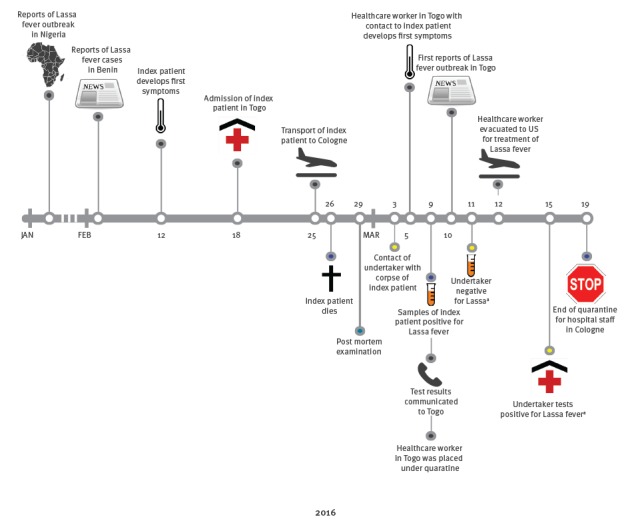
In a patient transferred from Togo to Cologne, Germany, Lassa fever was diagnosed 12 days post mortem. Sixty-two contacts in Cologne were categorised according to the level of exposure, and gradual infection control measures were applied. No clinical signs of Lassa virus infection or Lassa specific antibodies were observed in the 62 contacts. Thirty-three individuals had direct contact to blood, other body fluids or tissue of the patients. Notably, with standard precautions, no transmission occurred between the index patient and healthcare workers. However, one secondary infection occurred in an undertaker exposed to the corpse in Rhineland-Palatinate, who was treated on the isolation unit at the University Hospital of Frankfurt. After German authorities raised an alert regarding the imported Lassa fever case, an American healthcare worker who had cared for the index patient in Togo, and who presented with diarrhoea, vomiting and fever, was placed in isolation and medevacked to the United States. The event and the transmission of Lassa virus infection outside of Africa underlines the need for early diagnosis and use of adequate personal protection equipment (PPE), when highly contagious infections cannot be excluded. It also demonstrates that larger outbreaks can be prevented by infection control measures, including standard PPE.
在一名从多哥转诊至德国科隆的患者身上,尸检后12天确诊感染拉沙热。科隆的62名接触者根据接触程度进行了分类,并采取了逐步的感染控制措施。62名接触者中未观察到拉沙病毒感染的临床症状或拉沙特异性抗体。33人直接接触了患者的血液、其他体液或组织。值得注意的是,采取标准预防措施后,首例患者与医护人员之间未发生传播。然而,在莱茵兰-普法尔茨州一名接触尸体的殡仪员身上发生了一例继发感染,该患者在法兰克福大学医院隔离病房接受治疗。德国当局就输入性拉沙热病例发出警报后,一名曾在多哥照料首例患者、出现腹泻、呕吐和发热症状的美国医护人员被隔离,并通过医疗后送被送往美国。此次事件以及拉沙病毒感染在非洲以外地区的传播凸显出,在无法排除高传染性感染时,需要进行早期诊断并使用适当的个人防护装备(PPE)。这也表明,通过包括标准PPE在内的感染控制措施可以预防更大规模的疫情爆发。