Division of Nephrology, Department of Medicine.
Vanderbilt Center for Kidney Disease, and.
J Am Soc Nephrol. 2018 Jan;29(1):250-259. doi: 10.1681/ASN.2017010020. Epub 2017 Oct 16.
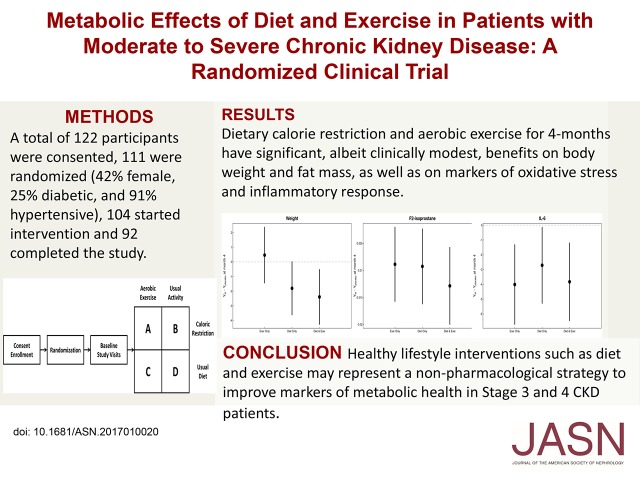
CKD is steadily increasing along with obesity worldwide. Furthermore, obesity is a proinflammatory risk factor for progression of CKD and cardiovascular disease. We tested the hypothesis that implementation of caloric restriction and aerobic exercise is feasible and can improve the proinflammatory metabolic milieu in patients with moderate to severe CKD through a pilot, randomized, 2×2 factorial design trial. Of 122 participants consented, 111 were randomized to receive caloric restriction and aerobic exercise, caloric restriction alone, aerobic exercise alone, or usual care. Of those randomized, 42% were women, 25% were diabetic, and 91% were hypertensive; 104 started intervention, and 92 completed the 4-month study. Primary outcomes were a change from baseline in absolute fat mass, body weight, plasma F-isoprostane concentrations, and peak oxygen uptake (VO). Compared with usual care, the combined intervention led to statistically significant decreases in body weight and body fat percentage. Caloric restriction alone also led to significant decreases in these measures, but aerobic exercise alone did not. The combined intervention and each independent intervention also led to significant decreases in F-isoprostane and IL-6 concentrations. No intervention produced significant changes in VO, kidney function, or urine albumin-to-creatinine ratio. In conclusion, 4-month dietary calorie restriction and aerobic exercise had significant, albeit clinically modest, benefits on body weight, fat mass, and markers of oxidative stress and inflammatory response in patients with moderate to severe CKD. These results suggest healthy lifestyle interventions as a nonpharmacologic strategy to improve markers of metabolic health in these patients.
慢性肾脏病(CKD)在全球范围内呈稳步上升趋势。此外,肥胖是 CKD 和心血管疾病进展的促炎危险因素。我们通过一项小型、随机、2×2 析因设计试验来检验以下假设,即限制热量摄入和有氧运动的实施是可行的,并能改善中重度 CKD 患者的促炎代谢环境。在 122 名同意参加的参与者中,111 名被随机分配接受热量限制和有氧运动、单独热量限制、单独有氧运动或常规护理。在随机分组的参与者中,42%为女性,25%患有糖尿病,91%患有高血压;104 人开始接受干预,92 人完成了 4 个月的研究。主要结局是从基线开始的绝对脂肪量、体重、血浆 F-异前列烷浓度和峰值摄氧量(VO)的变化。与常规护理相比,联合干预导致体重和体脂百分比有统计学意义的下降。单独热量限制也导致这些指标显著下降,但单独有氧运动则没有。联合干预和每个独立干预也导致 F-异前列烷和 IL-6 浓度显著下降。没有干预措施对 VO、肾功能或尿白蛋白/肌酐比值产生显著变化。总之,4 个月的饮食热量限制和有氧运动对中重度 CKD 患者的体重、体脂肪和氧化应激及炎症反应标志物有显著但临床意义不大的益处。这些结果表明,健康的生活方式干预是改善这些患者代谢健康标志物的非药物策略。