Division of Medical Oncology, Mayo Clinic, Rochester, Minnesota.
Alliance Statistics and Data Center, Mayo Clinic, Rochester, Minnesota.
Cancer. 2018 Feb 1;124(3):537-545. doi: 10.1002/cncr.31072. Epub 2017 Oct 17.
Despite the success of immune checkpoint and targeted therapy, many patients with melanoma ultimately require further treatment. The combination of carboplatin, paclitaxel, and bevacizumab (CPB) has demonstrated promising activity in a single-arm study. In the current study, the authors performed a randomized phase 2 study to confirm efficacy and to determine whether adding everolimus would increase the activity of the combination.
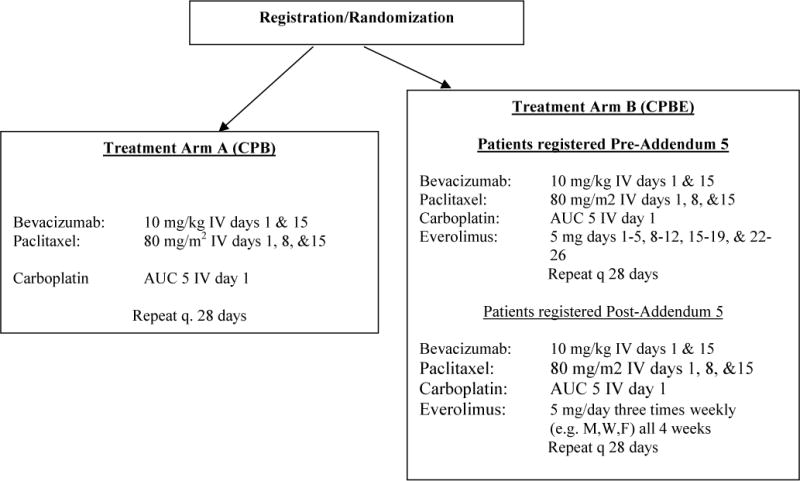
Through the North Central Cancer Treatment Group, a total of 149 patients with unresectable AJCC 6th edition stage IV melanoma were randomized from May 2010 to May 2014 to either CPB or CPB with everolimus (CPBE). The primary endpoint was progression-free survival (PFS), with secondary endpoints of overall survival (OS), response rate, and tolerability.
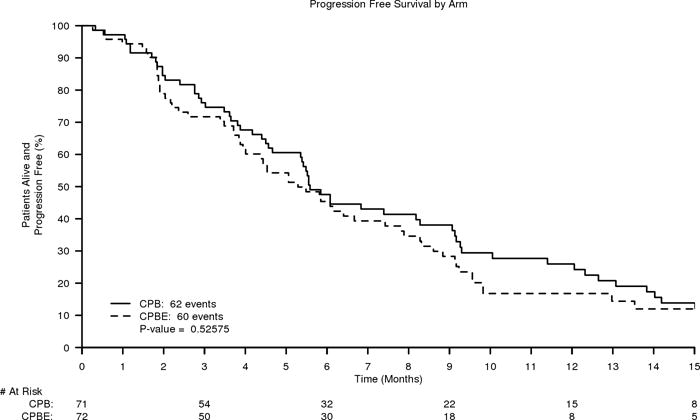
The CPB and CPBE treatment arms were balanced with regard to age (median age: 59 years vs 58 years) and high lactate dehydrogenase (48% vs 51%), but were unbalanced with regard to sex (male sex: 72% vs 55%; P = .03). Overall, there was no difference noted with regard to PFS, with a median PFS of 5.6 months for CPB versus 5.1 months for CPBE (hazard ratio [HR], 1.14; 95% confidence interval [95% CI], 0.81-1.62 [P = .44]), or for OS, with a median OS of 14.5 months for CPB versus 10.8 months for CPBE (HR, 1.16; 95% CI, 0.84-1.84). The confirmed response rate was 13% for CPB and 23% for CPBE (P = .13). Toxicity was higher for CPBE compared with CPB (83% for grade 3 + and 14% for grade 4 + vs 63% for grade 3 + and 11% for grade 4+, respectively) (toxicities were graded using the Cancer Therapy Evaluation Program of the National Cancer Institute Common Terminology Criteria for Adverse Events [version 4.0]). Common grade 3 + toxicities were neutropenia, leukopenia, and fatigue, which occurred in both treatment arms with comparable frequency.
Both experimental arms demonstrated activity, with a PFS of >5 months. However, the addition of everolimus to CPB failed to improve outcomes, with increased toxicity noted. These findings replicate the moderate antitumor activity of CPB, with future development possibly in combination with targeted or immunotherapy. Cancer 2018;124:537-45. © 2017 American Cancer Society.
尽管免疫检查点和靶向治疗取得了成功,但许多黑色素瘤患者最终仍需要进一步治疗。卡铂、紫杉醇和贝伐珠单抗(CPB)联合治疗在一项单臂研究中显示出了有前景的疗效。在目前的研究中,作者进行了一项随机 2 期研究,以确认疗效,并确定添加依维莫司是否会增加联合治疗的活性。
通过美国中部肿瘤协作组,共招募了 149 例无法切除的 AJCC 第 6 版 IV 期黑色素瘤患者,他们于 2010 年 5 月至 2014 年 5 月被随机分为 CPB 组或 CPB 联合依维莫司(CPBE)组。主要终点是无进展生存期(PFS),次要终点是总生存期(OS)、缓解率和耐受性。
CPB 和 CPBE 治疗组在年龄(中位年龄:59 岁比 58 岁)和高乳酸脱氢酶(48%比 51%)方面平衡,但在性别方面不平衡(男性:72%比 55%;P=0.03)。总体而言,CPB 和 CPBE 组之间的 PFS 没有差异,CPB 的中位 PFS 为 5.6 个月,CPBE 为 5.1 个月(HR,1.14;95%CI,0.81-1.62;P=0.44),OS 也没有差异,CPB 的中位 OS 为 14.5 个月,CPBE 为 10.8 个月(HR,1.16;95%CI,0.84-1.84)。CPB 的确认缓解率为 13%,CPBE 为 23%(P=0.13)。CPBE 组的毒性高于 CPB 组(3+级分别为 83%和 14%,4+级分别为 63%和 11%)(毒性采用国家癌症研究所癌症治疗评估计划的不良事件通用术语标准[版本 4.0]进行分级)。常见的 3+级毒性包括中性粒细胞减少症、白细胞减少症和疲劳,这两种治疗组的发生率相当。
两个实验组均表现出活性,PFS>5 个月。然而,CPB 联合依维莫司并不能改善疗效,且毒性增加。这些发现复制了 CPB 的中度抗肿瘤活性,未来的发展可能是联合靶向或免疫治疗。癌症 2018;124:537-45。©2017 美国癌症协会。