Department of Health Policy Planning and Management, Makerere University School of Public Health, Kampala, Uganda.
Department of Social Policy, London School of Economics and Political Science, London, UK.
Reprod Health. 2017 Oct 24;14(1):136. doi: 10.1186/s12978-017-0402-6.
The slow progress in reducing maternal and newborn death in low and middle-income countries is attributed to both demand and supply-side factors. This study assessed the changes in maternal and newborn services in health facilities as well as demand for maternal and newborn health services in Eastern Uganda.
The health assessment data were collected in August 2013 and September 2015 in the districts of Kamuli, Pallisa, and Kibuku. We purposively collected data on the availability of services from 40 health facilities that provided maternal and newborn services. In addition, we conducted 24 focus group discussions (FGDs) with women and men; and 18 key informant interviews (KIs) with health workers.
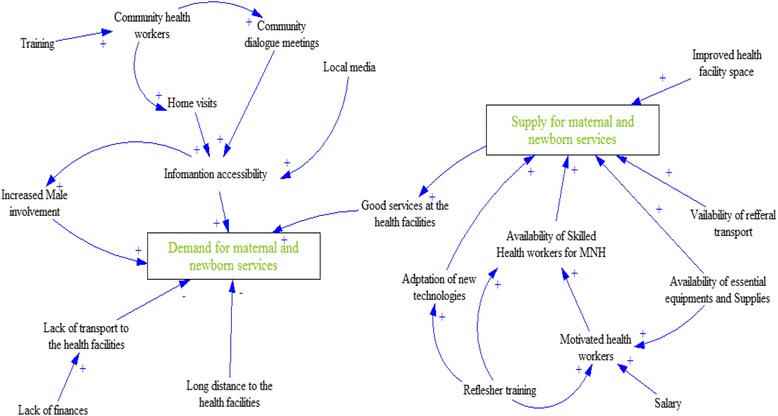
On the supply side, most health facilities persistently lacked lifesaving medicines such as misoprostol, IV Ampicillin, IV Gentamycin, IV Metronidazole, Magnesium Sulphate, Ergometrine, Corticosteroids, ferrous Sulphate, Folic Acid, Combined ferrous, Benzyl penicillin, and Diazepam (IM or IV). Basic newborn equipment such as stethoscope, fetal scope, working baby scale, newborn suction devices, newborn resuscitation device, and thermometer were persistently not available in most of the health facilities. Binders for Kangaroo Mother Care, blanket to wrap newborn, baby warmer or heat lamp were persistently not available in at least 80% of the health facilities. Other equipment for the management of labor and abortions such as Manual vacuum aspirator for abortion care, blank partographs and vacuum extractor were not available in most of the health facilities including referral facilities at baseline and follow-up. On the demand side, the qualitative interviews exposed long distances and inadequate transport to the health facilities, inadequate information, poverty, and poor services at the health facilities as major factors that impede women to utilize/access maternal and newborn services.
There are distinct influences on both demand and supply side, which restrain both health care uptake and its quality. The frequent disparity between the health facility readiness to provide services and the women readiness to utilize them needs to be addressed as the country intensifies its efforts to reduce maternal and newborn deaths through boosting facility deliveries.
中低收入国家在降低孕产妇和新生儿死亡率方面进展缓慢,这归因于供需两方面的因素。本研究评估了乌干达东部地区卫生机构中孕产妇和新生儿服务的变化情况,以及对孕产妇和新生儿卫生服务的需求情况。
2013 年 8 月和 2015 年 9 月在卡穆利、帕利萨和基布库地区收集了卫生评估数据。我们从提供孕产妇和新生儿服务的 40 个卫生机构中有意收集了服务提供情况的数据。此外,我们还对妇女和男子进行了 24 次焦点小组讨论(FGD),对卫生工作者进行了 18 次关键意见访谈(KII)。
在供应方面,大多数卫生机构持续缺乏米索前列醇、氨苄西林 IV、庆大霉素 IV、甲硝唑 IV、硫酸镁、麦角新碱、皮质类固醇、硫酸亚铁、叶酸、复合铁、苄星青霉素和地西泮(IM 或 IV)等救命药物。基本的新生儿设备,如听诊器、胎儿镜、工作婴儿秤、新生儿吸引器、新生儿复苏设备和温度计,在大多数卫生机构中持续无法获得。袋鼠式护理的固定器、包裹新生儿的毯子、婴儿保暖器或热灯,在至少 80%的卫生机构中持续无法获得。用于分娩和堕胎管理的其他设备,如手动流产吸引器用于堕胎护理、空白产程图和真空吸引器,在大多数卫生机构中都无法获得,包括基线和随访时的转诊机构。在需求方面,定性访谈揭示了距离远、交通不便、信息不足、贫困和卫生机构服务差等因素是阻碍妇女利用/获得孕产妇和新生儿服务的主要因素。
供需两方面都存在明显的影响,这限制了医疗保健的利用和质量。国家应加强努力,通过增加分娩来降低孕产妇和新生儿死亡率,因此需要解决卫生机构提供服务的准备情况与妇女利用服务的准备情况之间经常存在的差距。