Sharma Manuj, Beckley Nicholas, Nazareth Irwin, Petersen Irene
Department of Primary Care and Population Health, University College London, London, UK.
Department of Clinical Epidemiology, Aarhus University, Aarhus, Denmark.
BMJ Open. 2017 Oct 30;7(10):e017260. doi: 10.1136/bmjopen-2017-017260.
To assess the effectiveness of sitagliptin compared to sulfonylureas as add-on to metformin in adults with type 2 diabetes mellitus from both randomised controlled trials (RCTs) and 'real-world' non-randomised studies.
We conducted a systematic review of EMBASE, MEDLINE, CENTRAL and grey literature for RCTs and non-randomised studies. We reported outcomes relating to change in HbA1c, fasting glucose, weight, blood pressure and lipids from baseline and need for treatment change. No study investigating macrovascular and microvascular diabetes complications was found. Meta-analysis was used where studies were sufficiently homogenous.
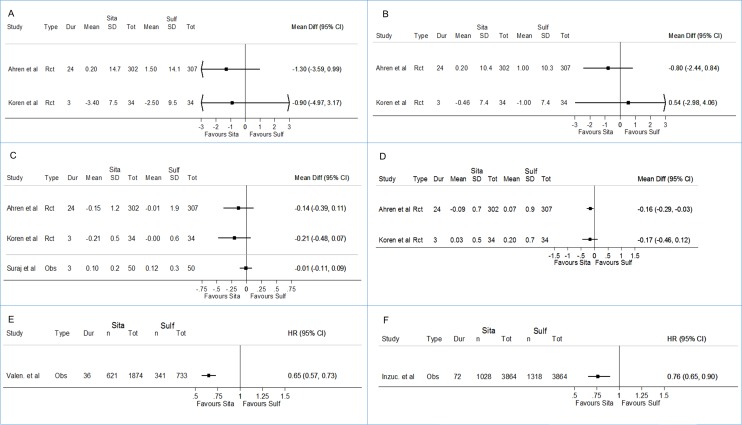
Seven RCTs and five non-randomised studies were eligible for inclusion from 1335 articles retrieved. Meta-analysis of three homogenous RCTs revealed a statistically significant decrease in weight with sitagliptin when compared to sulfonylureas (weighted mean difference (WMD) -2.05 kg; 95% CI -2.38 to -1.71); however, a similar change from baseline in HbA1c (WMD 0.05; 95% CI -0.03 to 0.12), fasting glucose (WMD 0.11; 95% CI -0.08 to -0.29), blood pressure, lipids and the proportion achieving HbA1c <7% by study end (OR 0.98; 95% CI 0.85 to 1.13) was observed.Non-randomised studies identified consisted of four prospective and one retrospective cohort study. Three of these five studies were of moderate/high quality, and results though less precise suggested similar real-world comparative glycaemic and weight effectiveness for both treatments. Data from two cohort studies suggested that treatment change (HR 0.65; 95% CI 0.57 to 0.73) and insulin initiation (HR 0.76; 95% CI 0.65 to 0.90) were less likely among those prescribed sitagliptin; however, inadequate reporting of HbA1c at time of treatment change made interpreting results challenging.
Sitagliptin users experienced modest weight loss compared to gain with sulfonylureas; however, this difference was around 2 kg, which may not be of major clinical significance for most individuals. Similar change was observed across most other effectiveness outcomes reported. Further studies are needed to address longer-term effectiveness outcomes for sitagliptin compared to sulfonylureas as add-on to metformin.
CRD42016033983.
通过随机对照试验(RCT)和“真实世界”非随机研究,评估与磺脲类药物相比,西格列汀作为二甲双胍附加治疗药物在2型糖尿病成人患者中的有效性。
我们对EMBASE、MEDLINE、CENTRAL数据库以及灰色文献进行了系统回顾,以查找RCT和非随机研究。我们报告了与糖化血红蛋白(HbA1c)、空腹血糖、体重、血压和血脂自基线起的变化以及治疗调整需求相关的结果。未找到研究大血管和微血管糖尿病并发症的研究。当研究足够同质时,使用荟萃分析。
从检索到的1335篇文章中,有7项RCT和5项非随机研究符合纳入标准。对3项同质RCT的荟萃分析显示,与磺脲类药物相比,西格列汀治疗后体重有统计学意义的下降(加权平均差(WMD)-2.05 kg;95%置信区间 -2.38至-1.71);然而,HbA1c(WMD 0.05;95%置信区间 -0.03至0.12)、空腹血糖(WMD 0.11;95%置信区间 -0.08至-0.29)、血压、血脂以及研究结束时HbA1c<7%的比例(比值比(OR)0.98;95%置信区间 0.85至1.13)自基线起的变化相似。所纳入的非随机研究包括4项前瞻性队列研究和1项回顾性队列研究。这5项研究中有3项质量为中/高,尽管结果不太精确,但表明两种治疗在真实世界中的血糖和体重比较有效性相似。两项队列研究的数据表明,使用西格列汀的患者进行治疗调整(风险比(HR)0.65;95%置信区间 0.57至0.73)和起始胰岛素治疗(HR 0.76;95%置信区间 0.65至0.90)的可能性较小;然而,治疗调整时HbA1c报告不充分,使得结果解读具有挑战性。
与使用磺脲类药物体重增加相比,使用西格列汀的患者体重适度减轻;然而,这种差异约为2 kg,对大多数个体可能不具有重大临床意义。在报告的大多数其他有效性结果中也观察到了类似变化。需要进一步研究以探讨与磺脲类药物相比,西格列汀作为二甲双胍附加治疗药物的长期有效性结果。
国际前瞻性注册系统(PROSPERO)注册号:CRD42016033983。