Staimez Lisa R, Wei Melissa Y, Kim Min, Narayan K M Venkat, Saydah Sharon H
Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, GA, USA.
Equal contribution.
J Comorb. 2017 Mar 13;7(1):22-32. doi: 10.15256/joc.2017.7.89. eCollection 2017.
Cardiometabolic and chronic pulmonary diseases may be associated with modifiable risk factors that can be targeted to prevent multimorbidity.
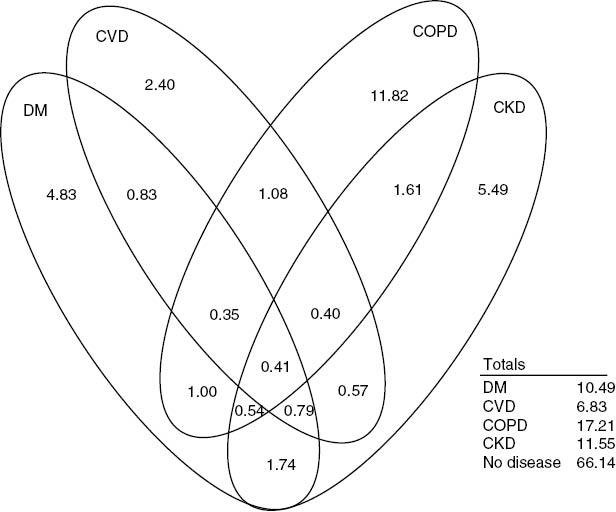
(i) Estimate the prevalence of multimorbidity across four cardiometabolic and chronic pulmonary disease groups; (ii) compare the prevalence of multimorbidity to that of one disease and no disease; and (iii) quantify population attributable fractions (PAFs) for modifiable risk factors of multimorbidity.
Data from adults aged 18-79 years who participated in the US National Health and Nutrition Examination Survey 2007-2012 were examined. Multimorbidity was defined as ≥2 co-occurring diseases across four common cardiometabolic and chronic pulmonary disease groups. Multivariate-adjusted PAFs for poverty, obesity, smoking, hypertension, and low high-density lipoprotein (HDL) cholesterol were estimated.
Among 16,676 adults, the age-standardized prevalence of multimorbidity was 9.3%. The occurrence of multimorbidity was greater with age, from 1.5% to 5.9%, 15.0% and 34.8% for adults aged 18-39, 40-54, 55-64 and 65-79 years, respectively. Multimorbidity was greatest among the poorest versus non-poorest adults and among blacks versus other races/ethnicities. Multimorbidity was also greater in adults with obesity, hypertension, and low HDL cholesterol. Risk factors with greatest PAFs were hypertension (38.8%; 95% confidence interval [CI] 29.4-47.4) and obesity (19.3%; 95% CI 10.2-28.2).
In the USA, 9.3% of adults have multimorbidity across four chronic disease groups, with a disproportionate burden among older, black, and poor adults. Our results suggest that targeting two modifiable risk factors, hypertension and obesity, might help to reduce the prevalence of multimorbidity in US adults.
心脏代谢疾病和慢性肺部疾病可能与可改变的风险因素相关,这些因素可作为预防多种疾病共存的目标。
(i)估计四个心脏代谢和慢性肺部疾病组中多种疾病共存的患病率;(ii)将多种疾病共存的患病率与单一疾病和无疾病的患病率进行比较;(iii)量化多种疾病共存的可改变风险因素的人群归因分数(PAF)。
研究了2007 - 2012年参加美国国家健康和营养检查调查的18 - 79岁成年人的数据。多种疾病共存定义为四个常见心脏代谢和慢性肺部疾病组中同时出现≥2种疾病。估计了贫困、肥胖、吸烟、高血压和低高密度脂蛋白(HDL)胆固醇的多变量调整PAF。
在16,676名成年人中,多种疾病共存的年龄标准化患病率为9.3%。多种疾病共存的发生率随年龄增长而增加,18 - 39岁、40 - 54岁、55 - 64岁和65 - 79岁成年人的发生率分别为1.5%至5.9%、15.0%和34.8%。最贫困与非最贫困成年人之间以及黑人与其他种族/族裔之间多种疾病共存情况最为严重。肥胖、高血压和HDL胆固醇低的成年人中多种疾病共存情况也更严重。PAF最高的风险因素是高血压(38.8%;95%置信区间[CI] 29.4 - 47.4)和肥胖(19.3%;95% CI 10.2 - 28.2)。
在美国,9.3%的成年人在四个慢性疾病组中存在多种疾病共存情况,老年、黑人及贫困成年人的负担不成比例。我们的结果表明,针对高血压和肥胖这两个可改变的风险因素,可能有助于降低美国成年人多种疾病共存的患病率。