Yeom Seul-Ki, Won Dong-Ok, Chi Seong In, Seo Kwang-Suk, Kim Hyun Jeong, Müller Klaus-Robert, Lee Seong-Whan
Department of Brain and Cognitive Engineering, Korea University, Seoul, Korea.
Department of Dental Anesthesiology, Seoul National University Dental Hospital, Seoul, Korea.
PLoS One. 2017 Nov 9;12(11):e0187743. doi: 10.1371/journal.pone.0187743. eCollection 2017.
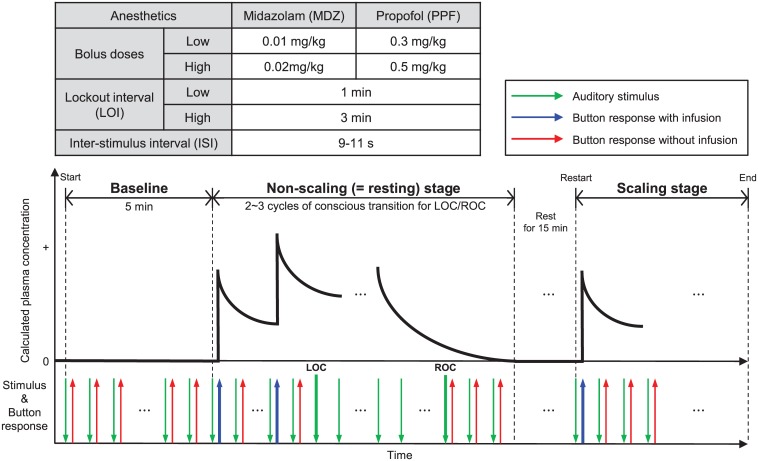
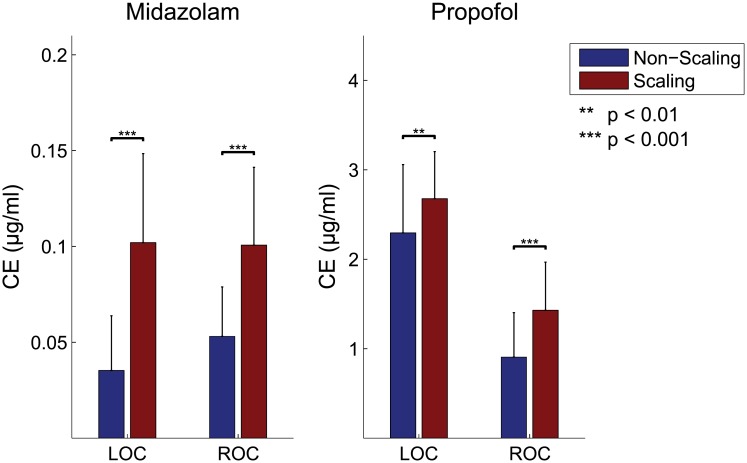
On sedation motivated by the clinical needs for safety and reliability, recent studies have attempted to identify brain-specific signatures for tracking patient transition into and out of consciousness, but the differences in neurophysiological effects between 1) the sedative types and 2) the presence/absence of surgical stimulations still remain unclear. Here we used multimodal electroencephalography-functional near-infrared spectroscopy (EEG-fNIRS) measurements to observe electrical and hemodynamic responses during sedation simultaneously. Forty healthy volunteers were instructed to push the button to administer sedatives in response to auditory stimuli every 9-11 s. To generally illustrate brain activity at repetitive transition points at the loss of consciousness (LOC) and the recovery of consciousness (ROC), patient-controlled sedation was performed using two different sedatives (midazolam (MDZ) and propofol (PPF)) under two surgical conditions. Once consciousness was lost via sedatives, we observed gradually increasing EEG power at lower frequencies (<15 Hz) and decreasing power at higher frequencies (>15 Hz), as well as spatially increased EEG powers in the delta and lower alpha bands, and particularly also in the upper alpha rhythm, at the frontal and parieto-occipital areas over time. During ROC from unconsciousness, these spatio-temporal changes were reversed. Interestingly, the level of consciousness was switched on/off at significantly higher effect-site concentrations of sedatives in the brain according to the use of surgical stimuli, but the spatio-temporal EEG patterns were similar, regardless of the sedative used. We also observed sudden phase shifts in fronto-parietal connectivity at the LOC and the ROC as critical points. fNIRS measurement also revealed mild hemodynamic fluctuations. Compared with general anesthesia, our results provide insights into critical hallmarks of sedative-induced (un)consciousness, which have similar spatio-temporal EEG-fNIRS patterns regardless of the stage and the sedative used.
出于对安全性和可靠性的临床需求而进行镇静时,最近的研究试图确定大脑特异性特征以追踪患者进入和脱离意识的转变过程,但1)镇静剂类型与2)手术刺激的有无之间的神经生理效应差异仍不清楚。在此,我们使用多模态脑电图-功能近红外光谱(EEG-fNIRS)测量来同时观察镇静过程中的电反应和血流动力学反应。40名健康志愿者被要求每9-11秒根据听觉刺激按下按钮自行给药。为了总体说明意识丧失(LOC)和意识恢复(ROC)时重复转变点的大脑活动,在两种手术条件下使用两种不同的镇静剂(咪达唑仑(MDZ)和丙泊酚(PPF))进行患者自控镇静。一旦通过镇静剂使意识丧失,我们观察到随着时间的推移,较低频率(<15Hz)的脑电图功率逐渐增加,较高频率(>15Hz)的功率逐渐降低,以及额叶和顶枕区的δ波和较低α波带,特别是上α节律的脑电图功率在空间上增加。在从无意识状态恢复意识(ROC)期间,这些时空变化被逆转。有趣的是,根据手术刺激的使用情况,大脑中镇静剂的效应部位浓度显著更高时意识水平会开启/关闭,但无论使用何种镇静剂,脑电图的时空模式相似。我们还观察到额叶-顶叶连接在LOC和ROC时的突然相位变化是关键点。fNIRS测量也显示出轻微的血流动力学波动。与全身麻醉相比,我们的结果为镇静诱导的(无)意识的关键特征提供了见解,无论阶段和使用的镇静剂如何,这些特征都具有相似的脑电图-fNIRS时空模式。