Jacobs Diane M, Ard M Colin, Salmon David P, Galasko Douglas R, Bondi Mark W, Edland Steven D
Department of Neurosciences, University of California, San Diego, La Jolla, CA, USA.
Shiley-Marcos Alzheimer's Disease Research Center, La Jolla, CA, USA.
Alzheimers Dement (N Y). 2017 Sep 19;3(4):531-535. doi: 10.1016/j.trci.2017.08.010. eCollection 2017 Nov.
Practice effects (PEs) present a potential confound in clinical trials with cognitive outcomes. A single-blind placebo run-in design, with repeated cognitive outcome assessments before randomization to treatment, can minimize effects of practice on trial outcome.
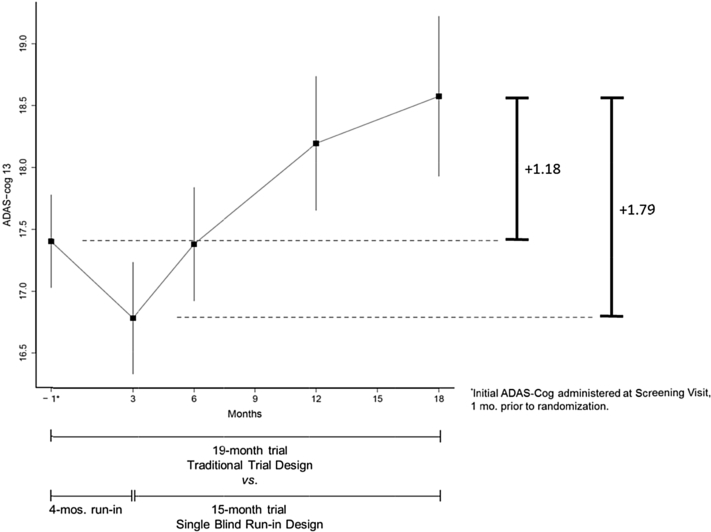
We investigated the potential implications of PEs in Alzheimer's disease prevention trials using placebo arm data from the Alzheimer's Disease Cooperative Study donepezil/vitamin E trial in mild cognitive impairment. Frequent ADAS-Cog measurements early in the trial allowed us to compare two competing trial designs: a 19-month trial with randomization after initial assessment, versus a 15-month trial with a 4-month single-blind placebo run-in and randomization after the second administration of the ADAS-Cog. Standard power calculations assuming a mixed-model repeated-measure analysis plan were used to calculate sample size requirements for a hypothetical future trial designed to detect a 50% slowing of cognitive decline.
On average, ADAS-Cog 13 scores improved at first follow-up, consistent with a PE and progressively worsened thereafter. The observed change for a 19-month trial (1.18 points) was substantively smaller than that for a 15-month trial with 4-month run-in (1.79 points). To detect a 50% slowing in progression under the standard design (i.e., a 0.59 point slowing), a future trial would require 3.4 times more subjects than would be required to detect the comparable percent slowing (i.e., 0.90 points) with the run-in design.
Assuming the improvement at first follow-up observed in this trial represents PEs, the rate of change from the second assessment forward is a more accurate representation of symptom progression in this population and is the appropriate reference point for describing treatment effects characterized as percent slowing of symptom progression; failure to accommodate this leads to an oversized clinical trial. We conclude that PEs are an important potential consideration when planning future trials.
在以认知结果为指标的临床试验中,练习效应(PEs)是一个潜在的混杂因素。采用单盲安慰剂导入设计,在随机分组接受治疗前进行多次认知结果评估,可将练习对试验结果的影响降至最低。
我们利用阿尔茨海默病合作研究多奈哌齐/维生素E试验中轻度认知障碍患者安慰剂组的数据,调查了练习效应在阿尔茨海默病预防试验中的潜在影响。在试验早期频繁进行阿尔茨海默病评定量表认知部分(ADAS-Cog)测量,使我们能够比较两种相互竞争的试验设计:一种是初始评估后随机分组的19个月试验,另一种是进行4个月单盲安慰剂导入、在第二次给予ADAS-Cog后随机分组的15个月试验。假设采用混合模型重复测量分析计划,使用标准功效计算来计算假设未来试验的样本量要求,该试验旨在检测认知衰退减缓50%的情况。
平均而言,首次随访时ADAS-Cog 13评分有所改善,这与练习效应一致,此后逐渐恶化。19个月试验的观察到的变化(1.18分)明显小于有4个月导入期的15个月试验(1.79分)。要在标准设计下检测到进展减缓50%(即减缓0.59分),未来试验所需的受试者数量将是采用导入设计检测到可比减缓百分比(即0.90分)所需受试者数量的3.4倍。
假设本试验中首次随访时观察到的改善代表练习效应,从第二次评估开始的变化率更准确地反映了该人群症状进展情况,并且是描述以症状进展减缓百分比为特征的治疗效果的合适参考点;未能考虑到这一点会导致临床试验规模过大。我们得出结论,在规划未来试验时,练习效应是一个重要的潜在考虑因素。