Longenecker Chris T, Morris Stephen R, Aliku Twalib O, Beaton Andrea, Costa Marco A, Kamya Moses R, Kityo Cissy, Lwabi Peter, Mirembe Grace, Nampijja Dorah, Rwebembera Joselyn, Sable Craig, Salata Robert A, Scheel Amy, Simon Daniel I, Ssinabulya Isaac, Okello Emmy
From the Case Western Reserve University School of Medicine, Cleveland, OH (C.T.L., S.R.M., M.A.C., R.A.S., D.I.S.); Division of Cardiovascular Medicine (C.T.L., M.A.C., D.I.S.) and Department of Medicine, University Hospitals Cleveland Medical Center, OH (S.R.M., R.A.S.); Uganda Heart Institute, Kampala, Uganda (T.O.A., P.L., J.R., I.S., E.O.); Department of Pediatric Cardiology, Children's National Health System, Washington, DC (A.B., C.S., A.S.); Department of Medicine, Makerere University School of Medicine, Kampala, Uganda (M.R.K.); Joint Clinical Research Centre, Kampala, Uganda (C.K., G.M.); and Mbarara University of Science and Technology, Mbarara, Uganda (D.N.)
From the Case Western Reserve University School of Medicine, Cleveland, OH (C.T.L., S.R.M., M.A.C., R.A.S., D.I.S.); Division of Cardiovascular Medicine (C.T.L., M.A.C., D.I.S.) and Department of Medicine, University Hospitals Cleveland Medical Center, OH (S.R.M., R.A.S.); Uganda Heart Institute, Kampala, Uganda (T.O.A., P.L., J.R., I.S., E.O.); Department of Pediatric Cardiology, Children's National Health System, Washington, DC (A.B., C.S., A.S.); Department of Medicine, Makerere University School of Medicine, Kampala, Uganda (M.R.K.); Joint Clinical Research Centre, Kampala, Uganda (C.K., G.M.); and Mbarara University of Science and Technology, Mbarara, Uganda (D.N.).
Circ Cardiovasc Qual Outcomes. 2017 Nov;10(11). doi: 10.1161/CIRCOUTCOMES.117.004037.
Rheumatic heart disease (RHD) is a leading cause of premature death and disability in low-income countries; however, few receive optimal benzathine penicillin G (BPG) therapy to prevent disease progression. We aimed to comprehensively describe the treatment cascade for RHD in Uganda to identify appropriate targets for intervention.
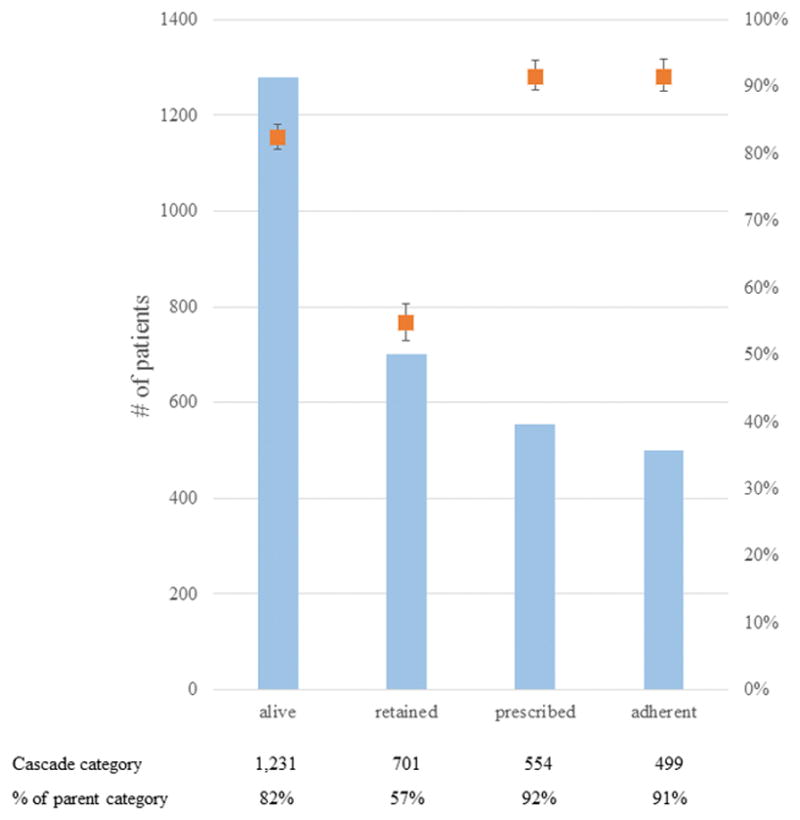
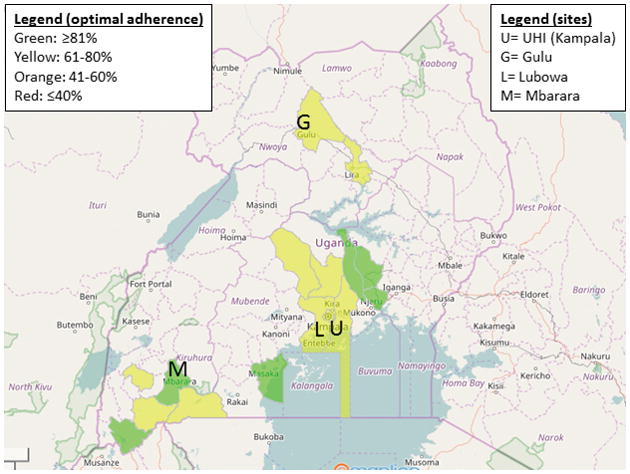
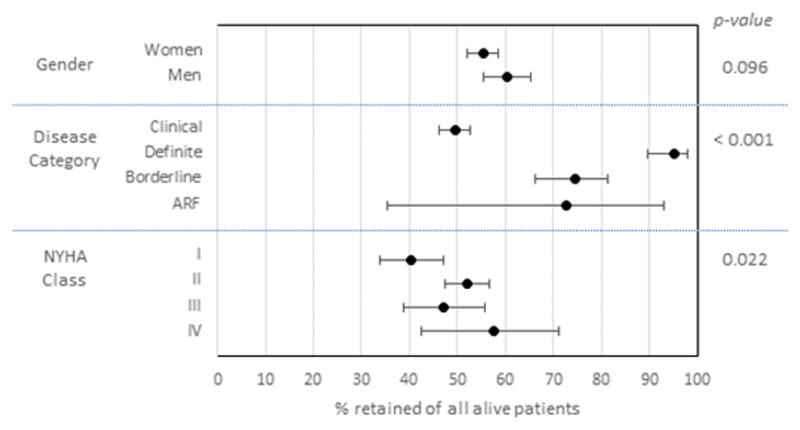
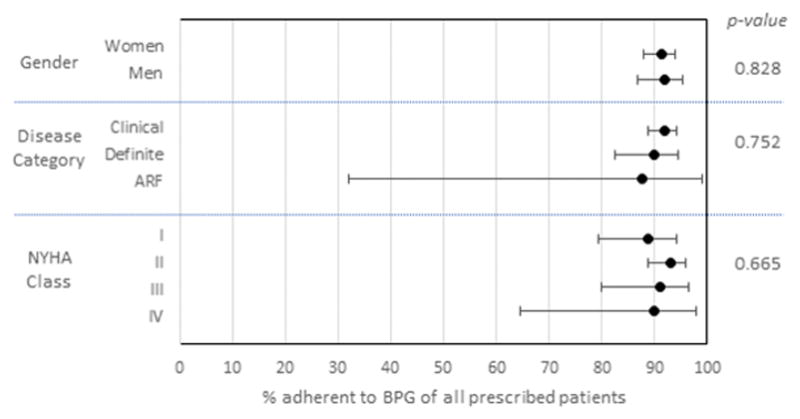
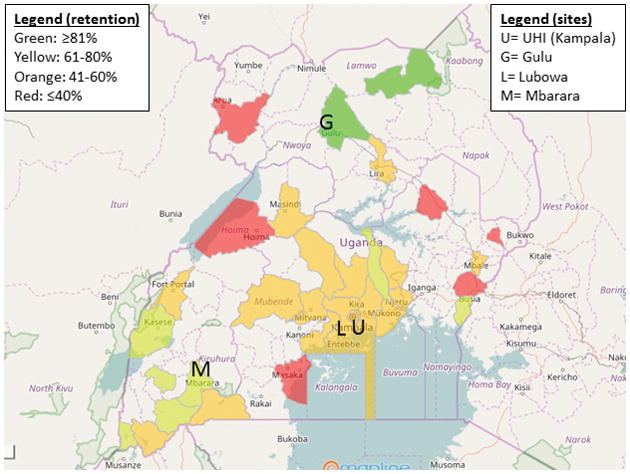
Using data from the Uganda RHD Registry (n=1504), we identified the proportion of patients in the following care categories: (1) diagnosed and alive as of June 1, 2016; (2) retained in care; (3) appropriately prescribed BPG; and (4) optimally adherent to BPG (>80% of prescribed doses). We used logistic regression to investigate factors associated with retention and optimal adherence. Overall, median (interquartile range) age was 23 (15-38) years, 69% were women, and 82% had clinical RHD. Median follow-up time was 2.4 (0.9-4.0) years. Retention in care was the most significant barrier to achieving optimal BPG adherence with only 56.9% (95% confidence interval, 54.1%-59.7%) of living subjects having attended clinic in the prior 56 weeks. Among those retained in care, however, we observed high rates of BPG prescription (91.6%; 95% confidence interval, 89.1%-93.5%) and optimal adherence (91.4%; 95% confidence interval, 88.7-93.5). Younger age, latent disease status, and access to care at a regional center were the strongest independent predictors of retention and optimal adherence.
Our study suggests that improving retention in care-possibly by decentralizing RHD services-would have the greatest impact on uptake of antibiotic prophylaxis among patients with RHD in Uganda.
风湿性心脏病(RHD)是低收入国家过早死亡和残疾的主要原因;然而,很少有人接受最佳的苄星青霉素G(BPG)治疗以预防疾病进展。我们旨在全面描述乌干达RHD的治疗流程,以确定合适的干预目标。
利用乌干达RHD登记处(n = 1504)的数据,我们确定了处于以下护理类别的患者比例:(1)截至2016年6月1日被诊断且存活;(2)持续接受护理;(3)适当开具BPG处方;(4)最佳依从BPG(>规定剂量的80%)。我们使用逻辑回归来研究与持续护理和最佳依从性相关的因素。总体而言,年龄中位数(四分位间距)为23(15 - 38)岁,69%为女性,82%患有临床RHD。中位随访时间为2.4(0.9 - 4.0)年。持续接受护理是实现最佳BPG依从性的最主要障碍,在前56周中只有56.9%(95%置信区间,54.1% - 59.7%)的存活患者到诊所就诊。然而,在持续接受护理的患者中,我们观察到BPG处方率很高(91.6%;95%置信区间,89.1% - 93.5%)且最佳依从率很高(91.4%;95%置信区间,88.7 - 93.5)。年龄较小、潜在疾病状态以及在区域中心获得护理是持续护理和最佳依从性最强的独立预测因素。
我们的研究表明,改善护理持续性(可能通过分散RHD服务)对乌干达RHD患者抗生素预防的采用率影响最大。